Presentation1, radiological film reading of knee joint.
•Download as PPTX, PDF•
21 likes•2,549 views

This document provides a radiological report and overview of knee pathology related to the meniscus and anterior cruciate ligament (ACL). It describes various grades of meniscal degeneration and discusses features of common meniscal tears including horizontal, longitudinal, radial, and bucket-handle tears. Anatomical variants like discoid meniscus are also reviewed. Expected MRI appearances of different tear patterns and signs like the double PCL sign for bucket-handle tears are presented. Healing responses and partial ACL tears are additionally summarized. The report contains multi-planar knee MRI images illustrating normal anatomy and various pathological conditions.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Presentation1, radiological film reading of knee joint.
Similar to Presentation1, radiological film reading of knee joint. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Presentation1, radiological film reading of knee joint.
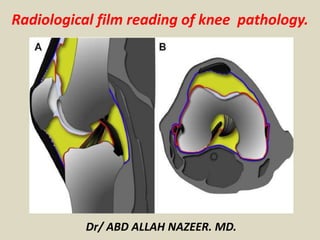
- 1. Radiological film reading of knee pathology. Dr/ ABD ALLAH NAZEER. MD.
- 5. Grade 1 myxoid degeneration of the Meniscus.
- 7. Grade 1 myxoid degeneration of the Meniscus.
- 9. Grade 11 myxoid degeneration of the Meniscus.
- 11. Grade 11 myxoid degeneration of the Meniscus.
- 13. Intrameniscal signal intensity into a medial meniscal tear over 48 months. Images show intrameniscal signal intensity grade 2 (arrowhead) at baseline, having progressed to grade 3 (arrowhead) at 24-month follow-up. At 48 months, the signal is visible on several sections and indicates a horizontal meniscal tear in the posterior horn (arrow).
- 14. Normal Anatomy Meniscal Tear. Normal meniscal anatomy. (a) Three-dimensional model (left) and cross-sectional diagram (right) of the semi lunar meniscus highlight the concave surface, which conforms to the morphology of the femoral condyles. The result is increased contact area and a tapered central free edge. Circumferentially oriented collagen bundles (blue cylinders) provide hoop strength and course parallel to the long axis of the meniscus, while radial fibers form a lattice and provide additional structural support. (b) Three-dimensional model shows the meniscus subdivided into thirds (the anterior horn [AH], body [B], and posterior horn [PH]) and attached to the tibia via the anterior and posterior root ligaments. Note the proximity of the roots to the tibial attachment sites for the anterior cruciate ligament (ACL) (black *) and posterior cruciate ligament (PCL) (white *). (c) Sagittal PD-weighted MR image shows the striated appearance of the anterior horn of the LM (arrow) due to contributing insertional fibers that originate from the ACL.
- 15. Normal meniscal anatomy. (a) Three- dimensional model (left) and cross-sectional diagram (right) of the semilunar meniscus highlight the concave surface, which conforms to the morphology of the femoral condyles. The result is increased contact area and a tapered central free edge. Circumferentially oriented collagen bundles (blue cylinders) provide hoop strength and course parallel to the long axis of the meniscus, while radial fibers form a lattice and provide additional structural support. (b) Three-dimensional model shows the meniscus subdivided into thirds (the anterior horn [AH], body [B], and posterior horn [PH]) and attached to the tibia via the anterior and posterior root ligaments. Note the proximity of the roots to the tibial attachment sites for the anterior cruciate ligament (ACL) (black *) and posterior cruciate ligament (PCL) (white *). (c) Sagittal PD- weighted MR image shows the striated appearance of the anterior horn of the LM (arrow) due to contributing insertional fibers that originate from the ACL.
- 16. Normal MR imaging appearance of the menisci. (a) Sagittal PD-weighted MR images show the typical bow-tie configuration of the meniscal body (left) and the opposing triangles of the horns (center and right). The posterior horn of the MM (arrow) is larger than the anterior horn, whereas the horns of the LM are similar in size and shape. (b) Coronal PD-weighted MR images demonstrate the triangular morphology of the meniscal body (left) and the elongated wedge shape of the posterior horn (right), which is continuous with the crescentic posterior meniscal root.
- 17. Normal MR imaging appearance of the menisci. (a) Sagittal PD-weighted MR images show the typical bow-tie configuration of the meniscal body (left) and the opposing triangles of the horns (center and right). The posterior horn of the MM (arrow) is larger than the anterior horn, whereas the horns of the LM are similar in size and shape. (b) Coronal PD-weighted MR images demonstrate the triangular morphology of the meniscal body (left) and the elongated wedge shape of the posterior horn (right), which is continuous with the crescentic posterior meniscal root.
- 18. Surrounding anatomy. (a) Sagittal PD-weighted MR image (left) shows an apparent anterior root tear (black arrow), which, when followed on multiple imaging sections and better depicted on the axial fluid-sensitive reconstructed MR image (right), is shown to be the normal transverse meniscal ligament (white arrow). (b) Sagittal PD-weighted MR image shows the Humphry (white arrow) and Wrisberg (black arrow) ligaments, which are located anterior and posterior to the PCL, respectively. (c) Sagittal T2-weighted MR image shows the posterosuperior (arrow) and anteroinferior (arrowhead) fascicles, which form the roof and floor of the popliteal hiatus, respectively. (d) Sagittal T2-weighted MR image obtained at a more medial level than c depicts the posteroinferior fascicle (arrow). Note the adjacent MFL (arrowhead). (e) Sagittal T2-weighted MR image shows a torn posterosuperior fascicle (arrow), which was found to be associated with an arthroscopically proved peripheral longitudinal LM tear. Note the “kissing” bone contusions from an ACL tear.
- 19. Anatomic variants. (a) Coronal fat-suppressed PD-weighted MR image through the body of the menisci shows a discoid LM (arrow) that measures 19 mm (normally <15 mm). (b) Sagittal PD-weighted MR image shows the typical rippled appearance of a meniscal flounce (arrowhead). (c) Sagittal PD-weighted MR image (left) shows marrow signal intensity within the MM posterior horn (black arrow), a finding that corresponds to a meniscal ossicle (white arrow) seen on the lateral radiograph (right).
- 20. Expected MR imaging appearance of a horizontal tear. (a) Three-dimensional model (center) shows a horizontal tear (arrow), and diagrams show the expected appearance of the tear on sagittal (left) and coronal (right) MR images. Dashed lines = orientation of imaging planes. (b) Sagittal T2-weighted MR image shows a tear of the posterior horn (arrow) and an associated multiloculated parameniscal cyst (arrowhead). (c) Coronal PD-weighted MR image shows a horizontal tear of the meniscal body (arrow) that contacts the superior articular surface.
- 21. Expected MR imaging appearance of a horizontal tear. (a) Three-dimensional model (center) shows a horizontal tear (arrow), and diagrams show the expected appearance of the tear on sagittal (left) and coronal (right) MR images. Dashed lines = orientation of imaging planes. (b) Sagittal T2- weighted MR image shows a tear of the posterior horn (arrow) and an associated multiloculated parameniscal cyst (arrowhead). (c) Coronal PD- weighted MR image shows a horizontal tear of the meniscal body (arrow) that contacts the superior articular surface.
- 23. Fat-suppressed proton density-weighted (4a) sagittal and (4b) coronal images reveal a horizontal tear of the posterior horn of the medial meniscus (arrows), extending to the tibial surface.
- 25. Horizontal tear of the posterior horn of the medial meniscus.
- 27. Horizontal tear of the posterior horn of the medial meniscus, extending to the tibial surface.
- 29. Horizontal tear of the posterior horn of the medial meniscus, extending to the tibial surface.
- 31. Horizontal tear of the lateral meniscus.
- 33. Horizontal flap tear: Graphic demonstrating displaced horizontal tear. Coronal and sagittal PD FS MR show displaced fragments in the posterior aspect of the joint near the PCL.
- 34. Longitudinal tear. (a) Three-dimensional model (left) and cross-sectional diagram (right) show a longitudinal tear (black arrows) extending to both articular surfaces, running along the long axis of the meniscus and dissecting it between the longitudinal collagen bundles (blue cylinders). A longitudinal tear separates the free edge from the periphery. (b) Arthroscopic image from Movie 1 shows a longitudinal tear parallel to the free edge. Inset shows the arthroscopic field of view.
- 35. Expected MR imaging appearance of a longitudinal tear. (a) Three-dimensional model (center) shows a typical longitudinal tear (arrow) that divides the meniscus into inner and outer halves, and diagrams show the expected appearance of the tear on sagittal (left) and coronal (right) MR images. Dashed lines = orientation of imaging planes. (b) Axial fluid-sensitive reformatted MR image shows a peripheral longitudinal tear involving the posterior body and posterior horn that extends into the posterior root arrows). (c) Sagittal PD-weighted MR image shows a peripheral longitudinal tear with increased intrasubstance signal intensity that unequivocally contacts the articular surface in a vertical orientation (arrow). This type of tear should not extend to the free edge.
- 37. Peripheral longitudinal tear extending to the tibial surface within the posterior horn of the medial meniscus.
- 39. Peripheral longitudinal tear extending to the articular surface within the posterior horn of the medial meniscus.
- 41. Vertical flap tars (Parrot-beak tears): Graphic and axial PD FS MR show an oblique radial (D) or longitudinal tear entering the free edge of the meniscus with displacement of the edge (A), resulting in a defect shaped like a parrot's beak or the letter "V” (B,C).
- 42. Radial (Root)tear. (a) Three-dimensional model (left) and cross-sectional diagram (right) show a radial tear (black arrows) that involves the free edge and is perpendicular to the long axis of the meniscus. The circumferential fibers responsible for resisting hoop strength are sequentially torn. Blue cylinders = longitudinal collagen bundles. (b) Arthroscopic image from Movie 2 shows a radial tear that involves the free edge. Inset shows the arthroscopic field of view.
- 43. MR imaging signs of a radial tear. Sagittal PD-weighted MR images demonstrate the cleft sign (arrowhead in a), the truncated triangle sign of a partial-thickness tear (arrowhead in b), and the ghost meniscus sign associated with a full-thickness tear (arrow in c). Each tear involves the free edge of the meniscus.
- 45. Marching cleft sign of a radial tear. (a) Sagittal PD-weighted contiguous MR images show a vertically oriented cleft (arrows) “marching” from the free edge into the substance of the meniscus at the junction of the body and anterior horn. (b) Axial fluid-sensitive reconstructed MR image shows the oblique course of a radial tear (arrow) with respect to the sagittal plane, which accounts for the MR imaging appearance of a tear propagating out of plane.
- 47. Complete root tear. (a, b) Coronal PD-weighted (a) and axial fluid-sensitive reconstructed (b) MR images show a complete posterior root tear (arrow).
- 51. (12a) A radial tear (arrow) truncates the central attachment/root of the posterior horn of the medial meniscus on this fat suppressed proton density-weighted coronal image. Associated medial subluxation of the meniscal body(arrow)
- 53. Radial tear with truncation of the posterior root of the medial meniscus. Axial, coronal and sagittal PD FS MR show meniscal extrusion (B) and the "ghost meniscus" sign of absent meniscal tissue (C).
- 57. Small radial tear of the lateral meniscus.
- 59. Radial tear of the posterior horn of the medial meniscus (small arrow). Wrisberg ligament
- 61. (16a) Sagittal and (16b) axial proton density weighted images reveal a very large radial tear (arrows) that extends broadly across the entire width of the anterior body of the lateral meniscus.
- 63. Complex tear. Sagittal PD-weighted MR image shows both vertical (arrowhead) and horizontal (arrow) components. Complex tears typically appear fragmented.
- 65. A GRE T2*-weighted sagittal image reveals a complex tear of the posterior horn of the medial meniscus, having horizontal (arrows) and longitudinal (arrowhead) components.
- 66. Bucket-handle tear. (a) Diagram shows a longitudinal tear (white arrow), with central displacement (red arrows) of the inner segment or “handle.” (b) Axial fluid-sensitive reconstructed MR image shows a rare bucket-handle tear that involves only about one-third of the meniscus (arrow). Typically this type of tear involves the majority of the meniscus.
- 68. Displaced tear. (a) Coronal T2-weighted MR image shows a flipped fragment within the intercondylar notch (arrow) from a complex tear of the MM. (b) Sagittal PD-weighted MR image shows a large flipped fragment (arrow) in the popliteal recess from a torn LM. (c) Coronal PD-weighted MR image (left) and corresponding anteroposterior radiograph (right) show a laterally displaced meniscal fragment (arrowheads) extending into the superior recess, with central areas of chondrocalcinosis.
- 70. MR imaging signs of a bucket-handle tear. (a) Sagittal PD-weighted MR image shows the absent bow-tie sign, with non- visualization of the meniscal body (arrows). (b) Sagittal PD-weighted MR image shows the fragment within the intercondylar notch sign, with a centrally displaced meniscal fragment (arrow) eccentric to the PCL. This finding is commonly seen with lateral tears because an intact ACL impedes the fragment from reaching the level of the PCL. (c) Sagittal PD-weighted MR image shows the double PCL sign, with a displaced fragment from the MM anterior and parallel to the PCL (arrow). (d) Sagittal PD-weighted MR image shows the double anterior horn sign, with a meniscal fragment (white arrow) posterior to and displacing the native anterior horn (black arrow) and a markedly diminutive posterior horn (arrowhead).
- 74. Fat-suppressed coronal images demonstrate before and after images following repair of a bucket handle tear. In (17a), the preoperative study, a large displaced "handle" (arrow) from the body of the lateral meniscus is seen near the intercondylar notch. Only a small peripheral rim of meniscal tissue (arrowhead) is present at the native site of the lateral meniscus.
- 76. Bucket-handle tear (BHT): Graphic, axial, coronal and sagittal PD FS MR show large intercondylar notch fragments (A-E), creating a "double PCL" sign anterior to the posterior cruciate ligament (D) and a “double delta” sign (D).Broken bucket- handle tear (E).
- 78. Flipped meniscus: Graphic, axial, coronal and sagittal PD FS MR show a lateral flipped meniscus. In this tear, a large portion of the posterior horn is displaced anteriorly and lies adjacent to the anterior horn. Notice the "double meniscus" sign (D,E). Severely truncated posterior horn (C, D, E).
- 80. Lateral Displaced Meniscal Bucket Handle Tear: MRI
- 82. Lateral Displaced Meniscal Bucket Handle Tear.
- 84. Lateral Displaced Meniscal Bucket Handle Tear.
- 86. (8a) The curvilinear course of oblique tears often results in abnormal vertical signal (arrows) that progresses towards or away from the free edge of the meniscus on consecutive images, as seen in these sequential images of an oblique tear (arrows) of the posterior horn of the medial meniscus.
- 91. Normal intrameniscal signal evolution in the site of surgery, with very good final result.
- 92. Normal healing sequence. Typical worsening in the first scans - intrameniscal signal after surgery is worse then before surgery. No healing disturbance.
- 93. Normal healing sequence. Typical worsening in the first scans - intrameniscal signal after surgery is worse then before surgery. Any of these scans without sequentional imaging would be difficult to differentiate from disturbed healing.
- 94. Abnormal healing of degenerated meniscus.
- 96. Partial tear of the proximal anteromedial band of the anterior cruciate ligament and tear of the medial collateral ligament. Anterior cruciate ligament.
- 98. A fat-suppressed proton-density sagittal view of an acute partial ACL tear depicts focal increased signal of the ACL (arrowheads) and a wavy contour of posterior fibers, which remain in continuity (arrow).
- 100. Partial ACL tear.
- 102. Partial ACL tear.
- 104. Partial ACL tear.
- 106. Partial tear of anterior cruciate ligament. Oblique sagittal T2-weighted MR shows diffuse high signal intensity within the ligament itself.
- 108. Sagittal T2 weighted image of partial anterior cruciate ligament (ACL) tear. The ACL appears lax and concave in appearance.
- 111. Partial ACL tear.
- 113. Partial tear of the ACL.
- 115. Partial ACL tear.
- 117. Sagittal T2W MRI demonstrates typical appearance of ACL tear at the mid-substance with fibres discontinuity of ACL.
- 119. Sagittal T2W MRI image demonstrates avulsion of ACL from tibial attachment.
- 121. LEFT: Acute ACL-tear. ACL fibers too flat compared to condylar roof. RIGHT: Discontinuity of fibers.
- 123. Primary signs of anterior cruciate ligament tear. Sagittal intermediate-weighted images of three different patients showing different patterns of anterior cruciate ligament (ACL) tear. A: Typical appearance of ACL tear at the mid-substance with fibres discontinuity of ACL (arrowheads). Residual stumps on femoral (asterisk) and tibial sides (white arrow) are lax, thickened and increased in signal intensity; B: Chronic ACL tear with absence of normal ACL fibres compatible with complete resorption of fibres. PCL (Curved black arrow); C: Acute high grade intrasubstance tear as characterized by thickening and edematous change of ACL fibres which show increased signal intensity (white arrows). The fibres are still in continuity suggestive of partial ACL tear.
- 125. (a) Normal sagittal image of ACL seen on 2 slices. The ligament is intact (green line) and parallels Blumesaat line (white line). (b-e) Sag PD images of different patients with complete ACL tear (red line). (b) ACL fibres are discontinuous, (c-d) different patients with mid ACL complete tear with flattened distal fibres. (e) Complete ACL tear with small bunched distal fibres. There is also complete tear of the proximal PCL (blue line).
- 127. (a) Sagittal T2-weighted MRI, complete disruption of the ACL fibres. (b) Avulsion of the tibial attachment of the ACL (arrows). (c) Same patient on CT.
- 128. PCL.
- 131. Partial PCL tear.
- 133. Multi-planar images showing partial high grade tear of the mid-distal PCL (red arrow).
- 135. Complete ACL tear and Partial PCL tear.
- 137. Sagittal PD & T2 FS MRI image demonstrates complete tear of PCL.
- 139. Complete PCL tear.
- 141. Complete PCL tear.
- 143. Complete PCL tear.
- 145. Sag PD images of 6 different patients with complete PCL tears (red line). Note is also made of complete ACL tears in all cases.
- 147. ACL Mucoid degeneration with cyst-formation (intra-osseous ganglion). Mucoid material is squeezed from between the ACL-fibers into the bone.
- 151. ACL ganglion cyst.
- 152. A 3-D cutaway at the intercondylar notch in the sagittal plane reveals normal positioning for a patellar tendon ACL autograft. The tibial tunnel should lie posterior to the line drawn parallel to the intercondylar notch (red) and the femoral attachment should lie posterior to a line drawn parallel to the cortex of the distal femoral diaphysis (blue).
- 154. The sagittal image reveals diffuse edema and abnormal laxity (arrows) along the course of the ACL graft, compatible with graft rupture. A displaced femoral fixation pin (arrowhead) is also apparent.
- 156. Femoral tunnel is normally positioned at the junction of the physeal scar and posterior intercondylar roof (asterisk). Abnormal placement of the femoral tunnel (asterisk), which lies significantly anterior to a line drawn along the posterior cortex of the femoral diaphysis with graft degeneration.
- 158. Tibial tunnel cyst after ACL graft reconstruction.
- 160. Cyclops lesion (arrowheads) attached to the ACL (arrow) with a head-like appearance, showing a focal area of discoloration resembling an eye (curved arrow)
- 162. Hypointense to isointense nodule (arrowhead) attached to the anterior surface of the anterior cruciate ligament (ACL) graft (arrow). Sagittal T1W MRI image (C) shows a hypointense nodule (arrowhead) in the anterior intercondylar notch, related to Cyclops.
- 164. ACL reconstruction are provided. Diffuse abnormal fluid signal intensity is seen along the course of the graft (arrows) on the sagittal image, compatible with extensive graft ganglion formation.
- 166. ACL Surgery Failure with stem cells injection.
- 168. Grade 1 MCL Sprain. Collateral ligaments.
- 170. Grade II MCL Sprain
- 172. Cor PD images of 3 patients showing thickened MCL with some disruption of fibres proximally in keeping with partial tears.
- 174. Cor PD images of different patients with complete distal MCL tear. Top left image shows complete disruption of distal fibres (yellow arrow). Top right and bottom left images show complete MCL tear with retracted and coiled up MCL (red arrow), tear of the medial meniscus is also seen (black arrow). Bottom right image shows complete discontinuity of MCL with hemorrhage (orange arrow) with muscle tears and hematoma in vastus lateralis (yellow star).
- 176. Superficial MCL-tear (yellow arrow) and deep MCL tear (orange arrow).
- 180. LEFT: distal rupture of fibular collateral ligament. RIGHT: biceps femoris tendon and collateral ligament do not attach.
- 182. Posterolateral corner injury with complete tear of the lateral collateral ligament (blue arrow) and biceps tendon (white arrow). There is also avulsion of the popliteal tendon (not shown) with muscle edema (red star). There is fluid decompressed out of the lateral side of the knee joint into the subcutaneous tissues and interfacial plane (yellow star).
- 183. Patellar retinaculum
- 184. Complete tear of the medial patellar retinaculum with defect (white arrow) with retracted fibres in the patellofemoral compartment (yellow arrow). There is also a partial tear of the lateral patellar retinaculum (orange arrow) with lateral femoral condyle contusion (red star) and fascial edema (blue arrow). Patellar retinaculum
- 186. Ax PD FS images (a) with complete medial patellar retinaculum tear (red arrow) and capsular disruption (orange star). (b) Shows complete lateral patellar retinaculum and iliotibial band tear (orange arrow) with capsular disruption (orange star). Bony contusions are seen on the contralateral femoral condyle (yellow star).
- 188. Iliotibial Band Friction syndrome: no fat between iliotibial band (yellow arrow) and the lateral condyle.
- 190. Cor PD images from 3 different patients showing complete iliotibial band tear (red arrow) with capsular disruption (orange star)
- 192. Patellar tendinosis.
- 194. A sagittal T2 fat sat image depicts a high grade partial tear of the quadriceps tendon. The distal edge (red arrow) of the tendon is well seen, as is the large hematoma (green arrow). The patella (pink arrow) is positioned more inferiorly than normal, and the patellar tendon (white arrow) is lax, suggesting that this is functionally a complete tear. The deep layer of the quadriceps tendon, composed of the vastus intermedius (yellow arrow), remains intact.
- 196. Partial quadriceps tendon tear: T2W-images.LEFT: Abnormal attachment of tendon. RIGHT: Most of tendon is retracted (red arrow) deep part (vastus intermedius) is still intact.
- 198. LEFT: Torn tendon with pre-existing tendinopathy (red arrow). RIGHT: Intact vastus intermedius tendon.
- 200. LEFT: Partial quadriceps tear. Only rectus femoris tendon is torn (blue arrow). RIGHT: Pre-existing tendinopathy (yellow circle) on axial image.
- 202. The quadriceps tendon attaches to the superior aspect of the patella and, together with the quadriceps muscles of the thigh and the patellar ligament, allows knee extension. Strains and overuse injuries to the quadriceps tendon are common and result in microscopic tears and inflammation. Following a quadriceps tendon injury, patients may or may not be able to ambulate. Tendon rupture can be manifested as abnormal thickening of the tendon (left image) or as complete, revealing retraction of the quadriceps tendon (right image). Individuals with a complete tear will be unable to extend the knee and often have a palpable defect at the site of tendon rupture. Initial management consists of immobilization, crutches, rest, ice, and elevation. Complete tendon rupture requires surgical repair.
- 204. A, B, Sagittal MRI scans demonstrating a quadriceps tendon tear at the osteotendinous junction.
- 206. Simultaneous Bilateral Quadriceps Tendon Rupture in Patient with Chronic Renal Failure.
- 210. Complete quadriceps tear. Sag T2W-images. No continuity. Hematoma in between.
- 212. Patellar tendinopathy and Partial patellar tendon tear.
- 214. Complete Patellar tendon tear. Image on the right shows hemorrhagic bursitis ( low signal in bursa).
- 216. Patellar sleeve avulsion. Fracture line only visible on the coronal images.
- 218. LEFT: Bone bruise lateral condyle (yellow circle). Normal MCL (green arrow) but missing patellar femoral ligament anterior to it. RIGHT: Medial patellar femoral ligament thorn from femoral attachment.
- 220. LEFT: Bone bruise medial patella (green arrow).RIGHT: Cartilage fracture.
- 242. Osgood-Schlutter disease. A, Lateral radiograph. B, Proton density sagittal image of the knee demonstrates tibial tuberosity fragmentation. C, A T2-weighted fat suppression sagittal image demonstrates edema of the tibial fragmentation (arrow) and adjacent Hoffa’s fat pad.
- 249. Stable Osteochondritis Dissecans. Stable Osteochondritis Dissecans with arthrogram.
- 257. Prepatellar bursitis
- 260. Superficial infrapatellar bursitis. A 42-year-old female presented with an anterior knee swelling. Sagittal proton-density fat saturated (A) and sagittal gradient-echo T2W (B) images show a distended superficial infrapatellar bursa (arrows)
- 264. Suprapatellar bursitis. A 29-year-old male presented with internal derangement of the knee: sagittal proton density fat saturated (A) and axial T2W gradient-echo (B) images show a distended suprapatellar bursa (arrows) and in addition, a partial tear of the anterior cruciate ligament (thick arrow in A)
- 266. Medial collateral ligament bursitis located between the deep MCL (yellow arrow) and the superficial MCL (green arrow).
- 268. Medial collateral ligament bursitis. A 54-year-old female presented with knee swelling: sagittal true inversion recovery magnitude (TIRM) (A) and axial T2W (B) images show a distended medial collateral ligament burse (arrows)
- 270. Pes anserine bursitis. A 32-year-old female presented with pain along the posteromedial aspect of the knee: Coronal proton density (A) and axial T2W (B) images show a distended pes anserine bursa (arrows). The pes anserinus tendons (arrowhead in B) are seen inferior to the bursa
- 272. Ilio-tibial bursitis with distended ilio-tibial bursa.
- 274. Baker's cyst. A 48-year-old male presented with swelling in the popliteal fossa: sagittal (A) and axial (B) T2W gradient-echo images show a distended gastrocnemius--semimembranosus bursa (arrows).
- 284. Infrapatellar (Hoffa’s fat pad) ganglion cyst arising from the anterior cruciate ligament.
- 286. Large infrapatellar ganglionic cyst of the knee fat pad.
- 288. T1-weighted sagittal and (9b) proton density-weighted axial images demonstrate a large, fluid signal intensity mass (arrows) which fills the infrapatellar fat pad in this patient who presented with palpable anterior knee swelling. The well-defined, homogeneous appearance of the lesion is typical for a benign ganglion, but in light of lesion size, intravenous contrast was administered
- 290. Ganglion cyst of the ACL.
- 292. Ganglion cyst of the PCL.
- 294. Patella Alta and Baja.
- 296. Patella Alta. Measurement of the Insall-Salvatti Index on Sagittal 2D GE MRI images of the left (6a) and right (6b) knees of the patient in the unknown case demonstrates ISI values which are diagnostic of patella alta.
- 298. Patella Baja. Demonstration of an abnormal MRI Insall-Salvatti Index measurement on a patient with patella baja (7a). The patient in 7b and 7c is post operative tibial tubercle transfer and demonstrates thickening of the patellar tendon insertion (arrows) and scarring in the infrapatellar fat pad (asterisk) (7b) and an abnormal MRI Insall-Salvatti Index of 0.51 (7c) which is diagnostic of patella baja.
- 300. Thank You.