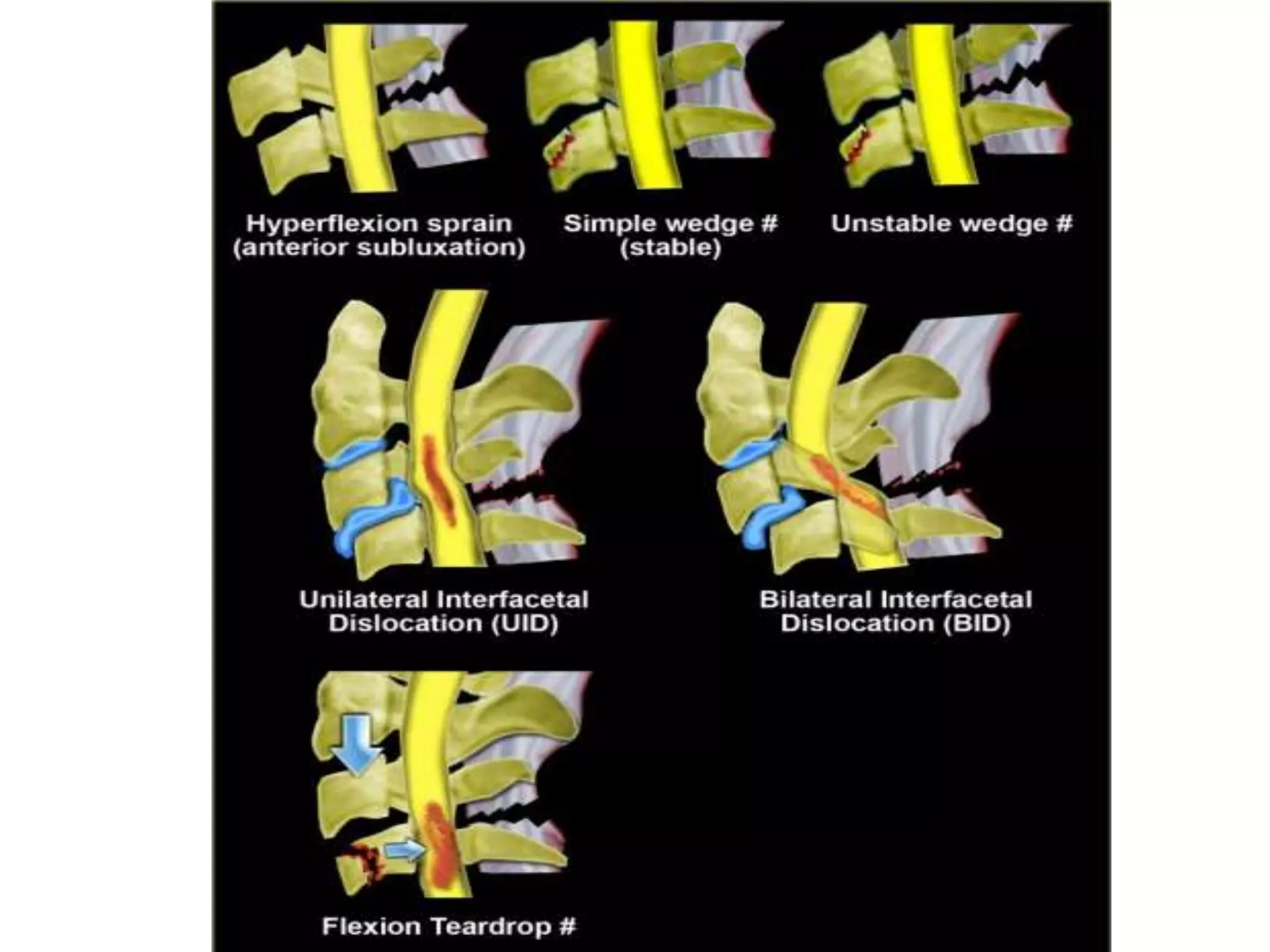
The document discusses various types of cervical spine trauma and injuries that can occur. It describes fractures of the atlas including Jefferson's fracture and posterior arch fractures. Hangman's fractures and teardrop fractures of the axis are also summarized. Odontoid fractures are divided into Types I-III. Vertebral body compression fractures like wedge fractures and burst fractures are mentioned. The document also briefly summarizes clay shoveler's fractures and lamina and transverse process fractures of the cervical spine. Various imaging modalities for evaluating cervical spine injuries are also discussed.