Downloaded 271 times

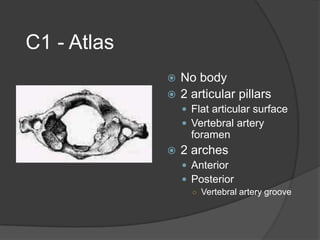
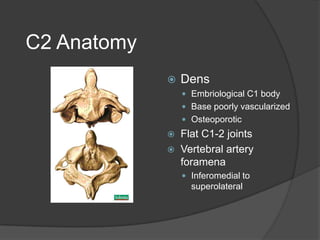
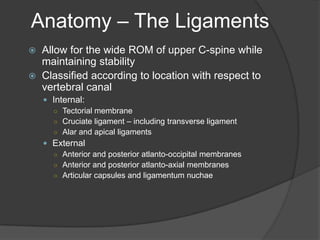
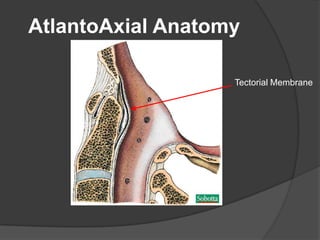
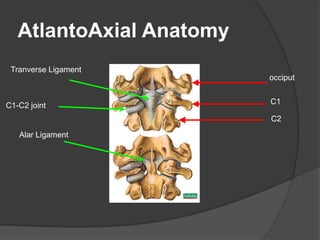
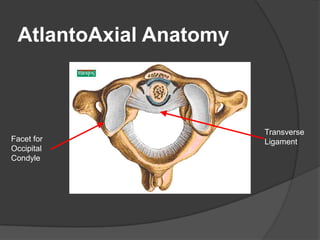
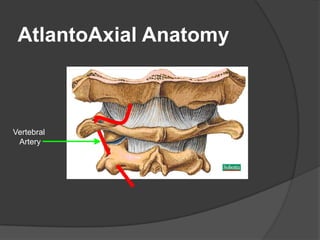
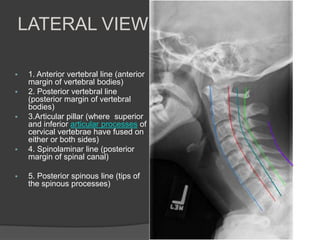
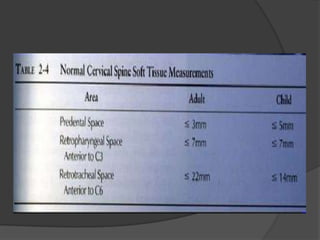
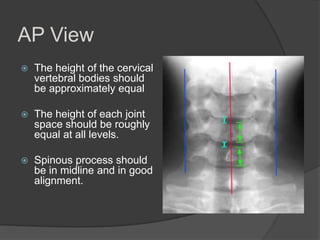
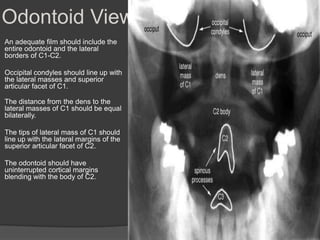
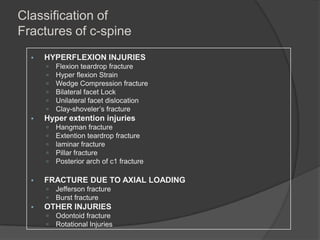
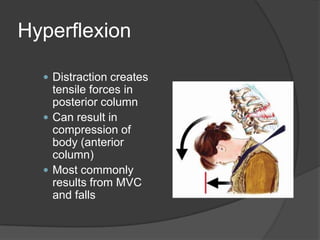
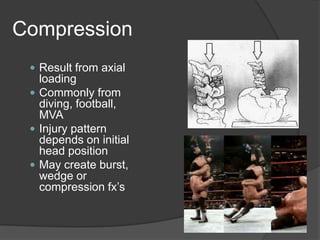
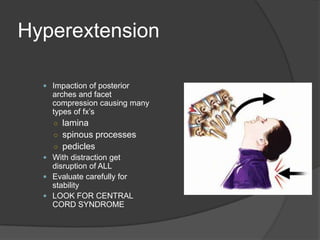
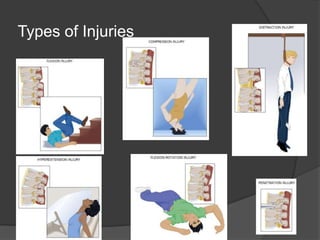
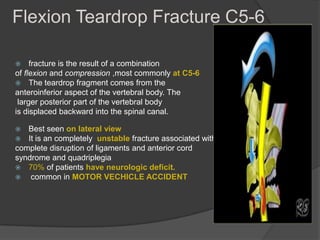
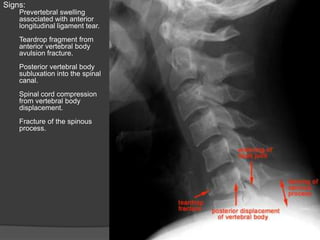
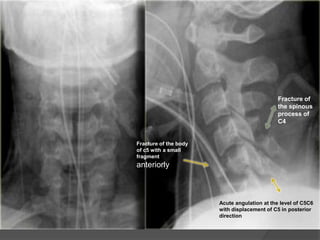
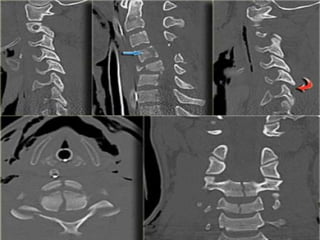


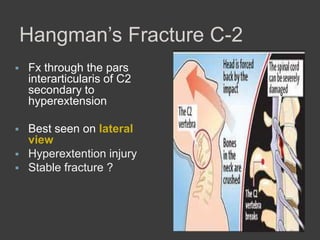
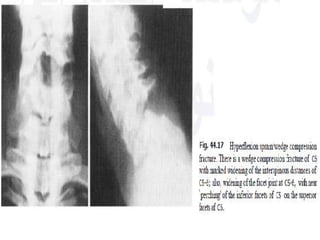
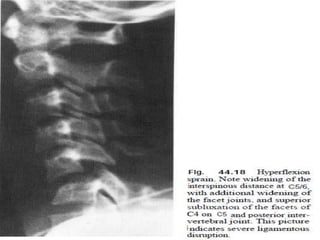
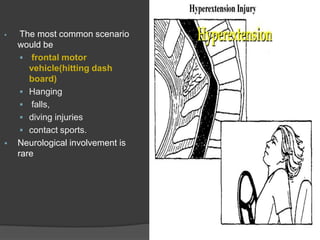







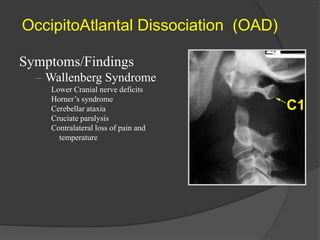



The cervical spine anatomy is specialized to support the cranium while allowing a large range of motion. C1 (atlas) has no vertebral body and unique articular pillars. C2 (axis) has a dens that is embryologically derived from C1's body. The ligaments of the cervical spine, including the tectorial membrane and transverse ligament, allow for wide range of motion while maintaining stability. Common cervical spine injuries include flexion teardrop fractures from hyperflexion, wedge fractures from compression, hangman's fractures from hyperextension, and Jefferson fractures from axial loading. Odontoid fractures also occur from hyperextension or hyperflexion forces on the neck. Radiographic evaluation of









































































