Downloaded 188 times
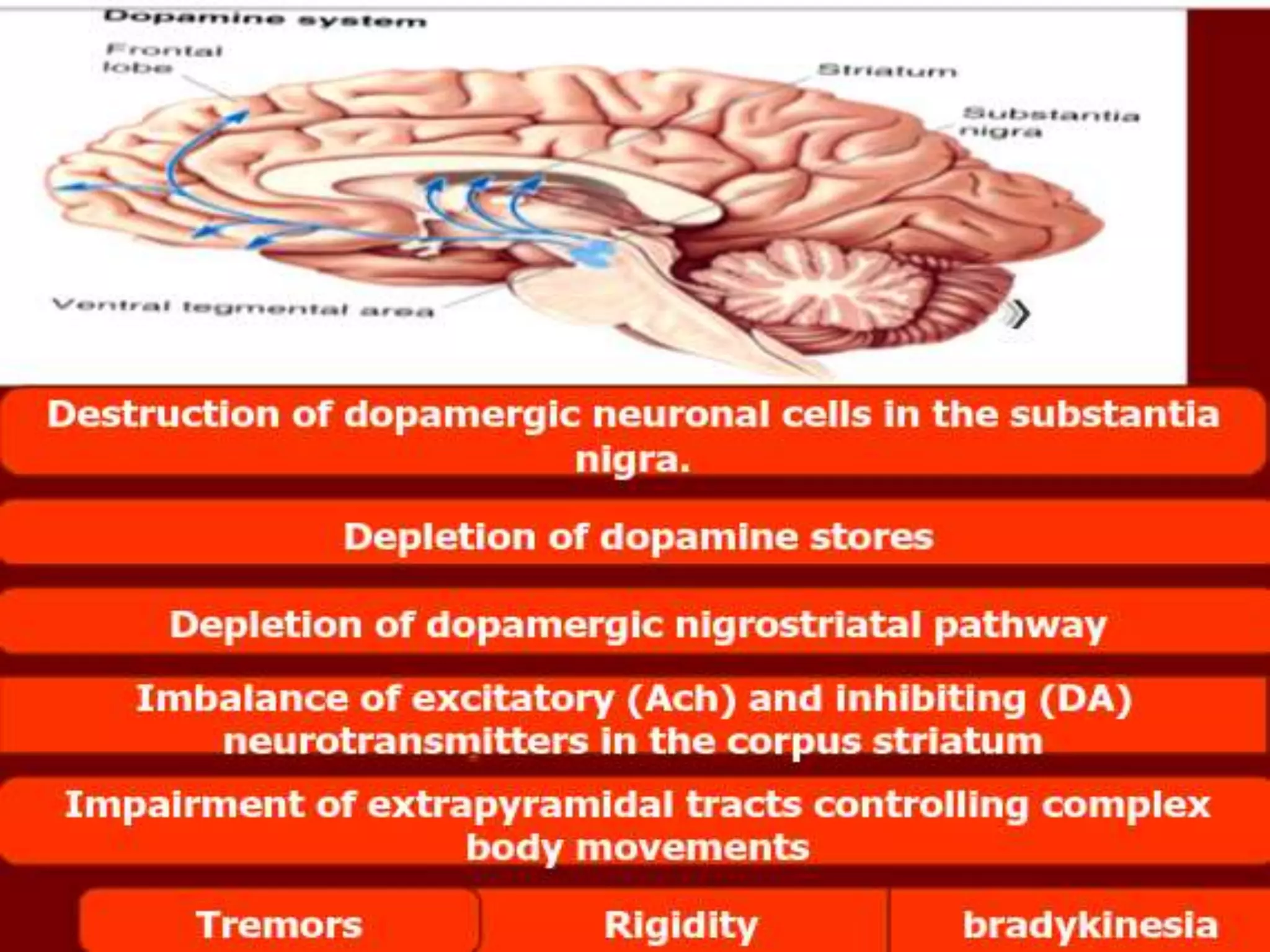
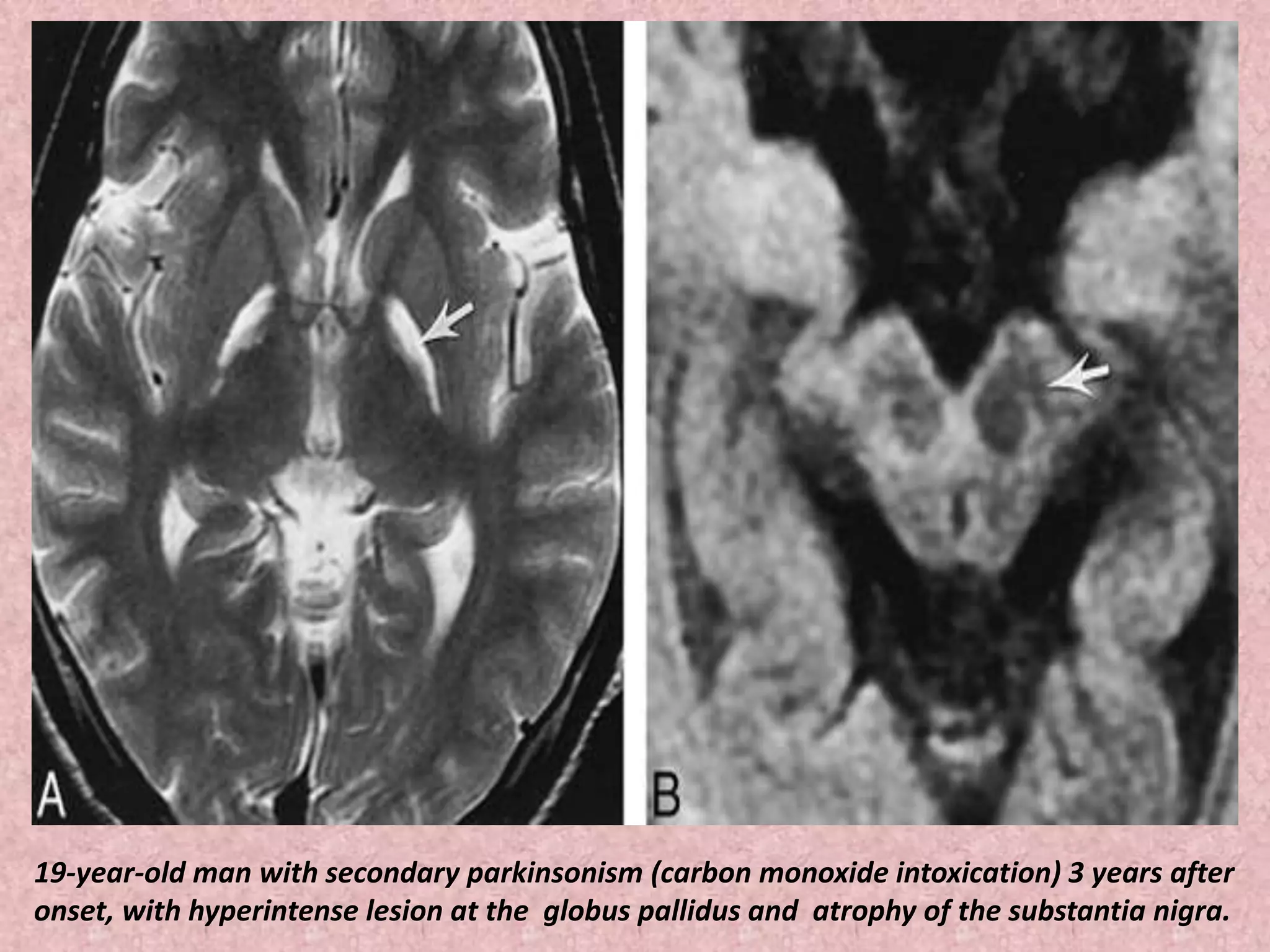
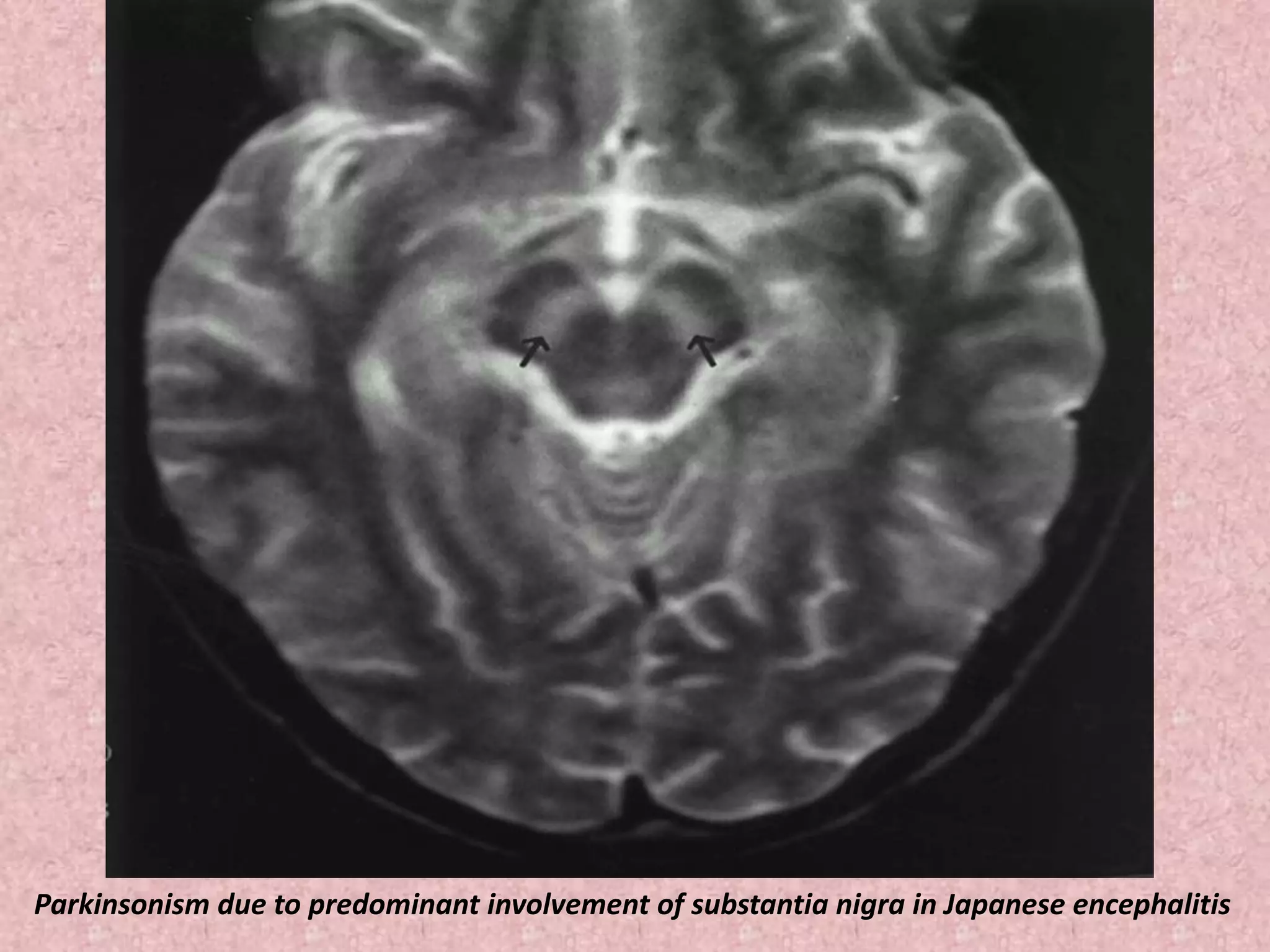
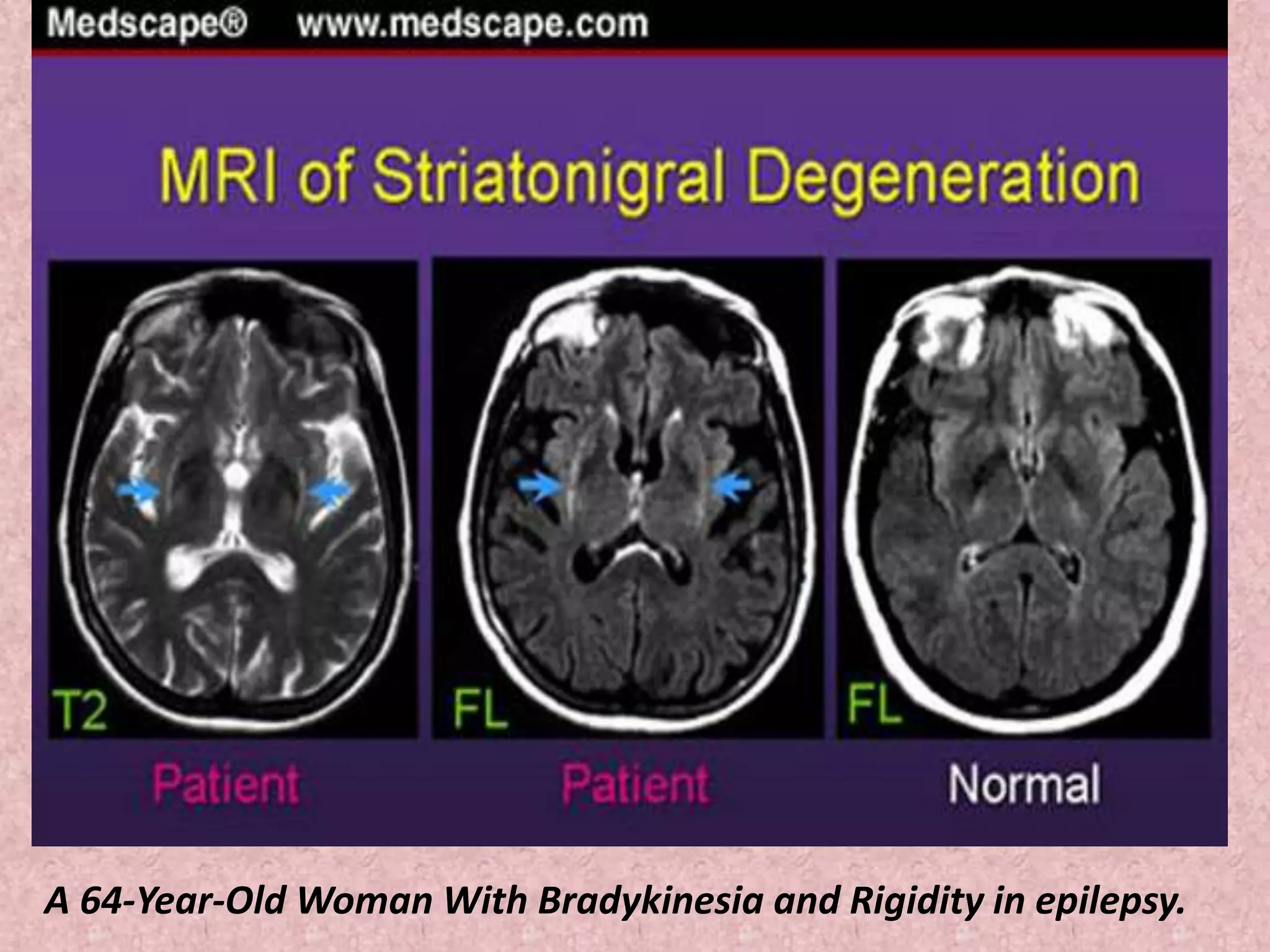
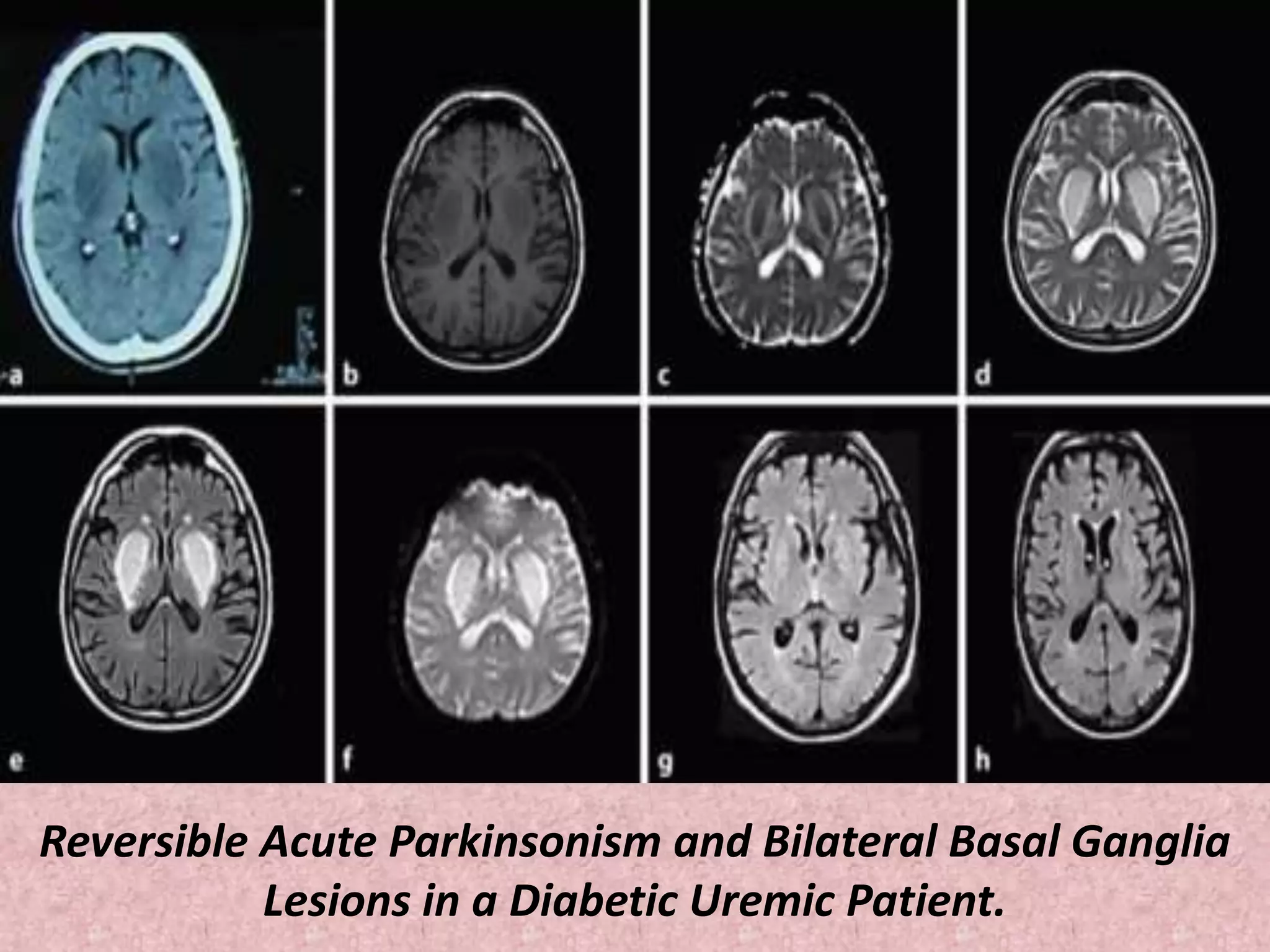
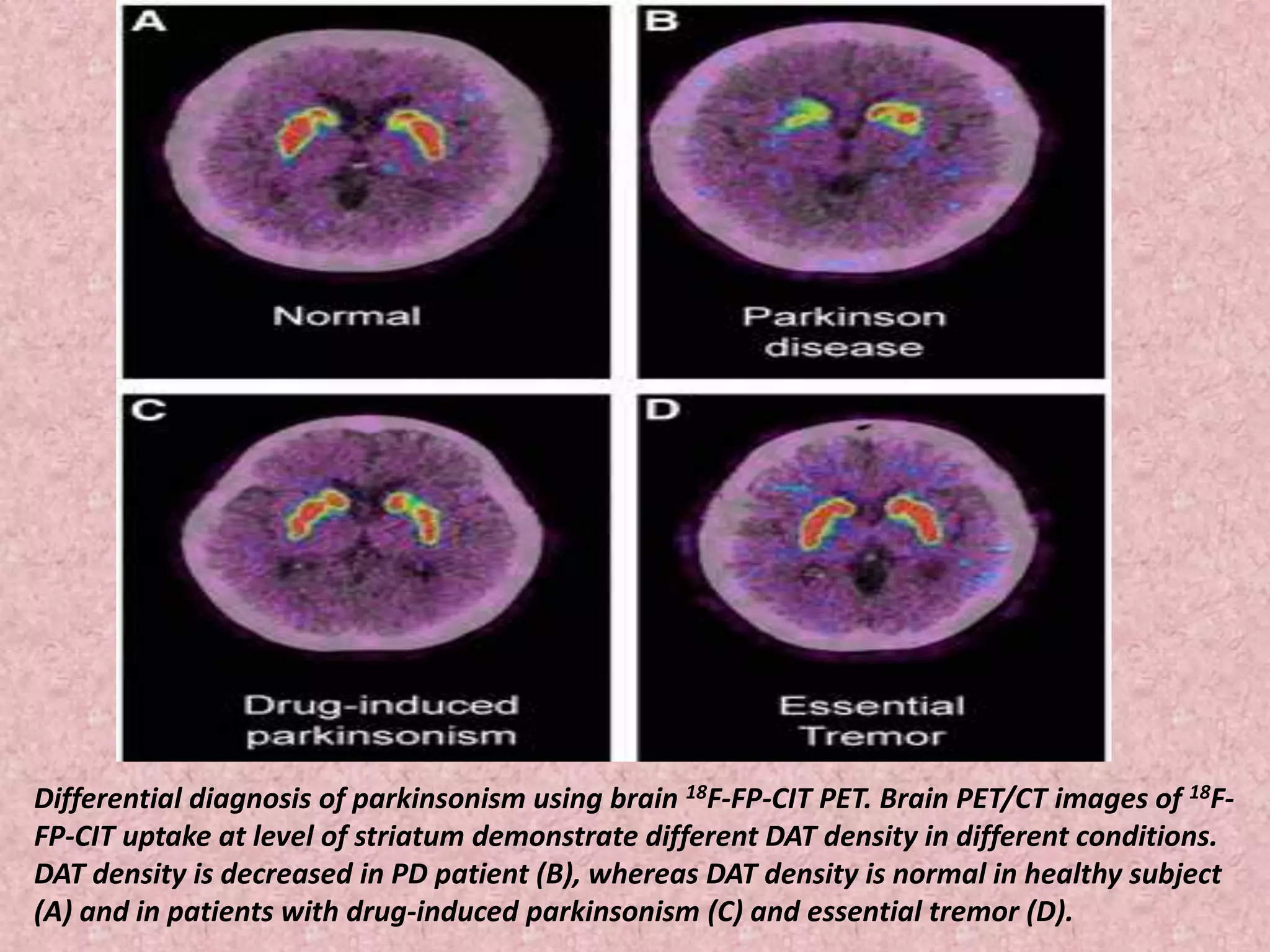
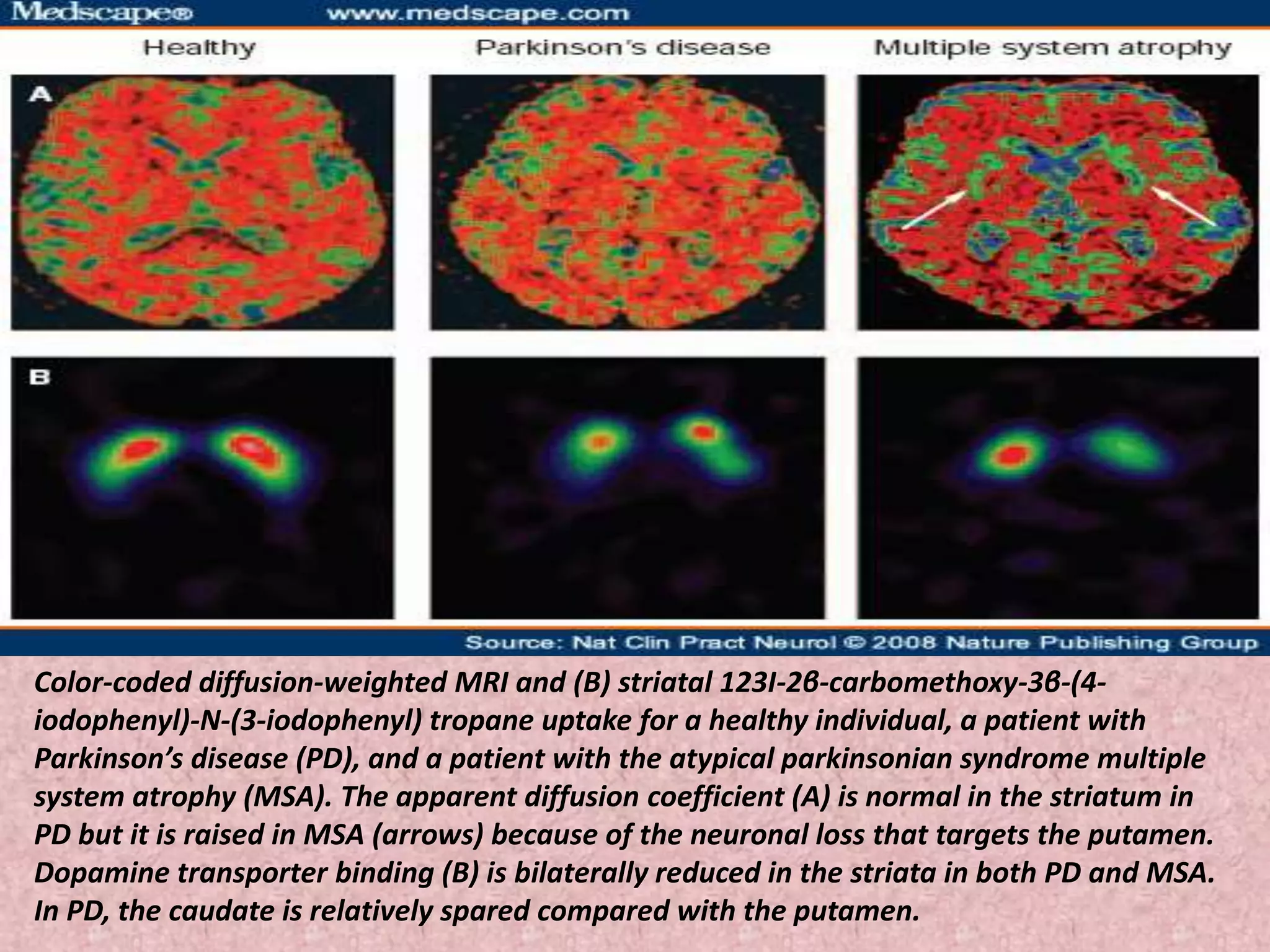
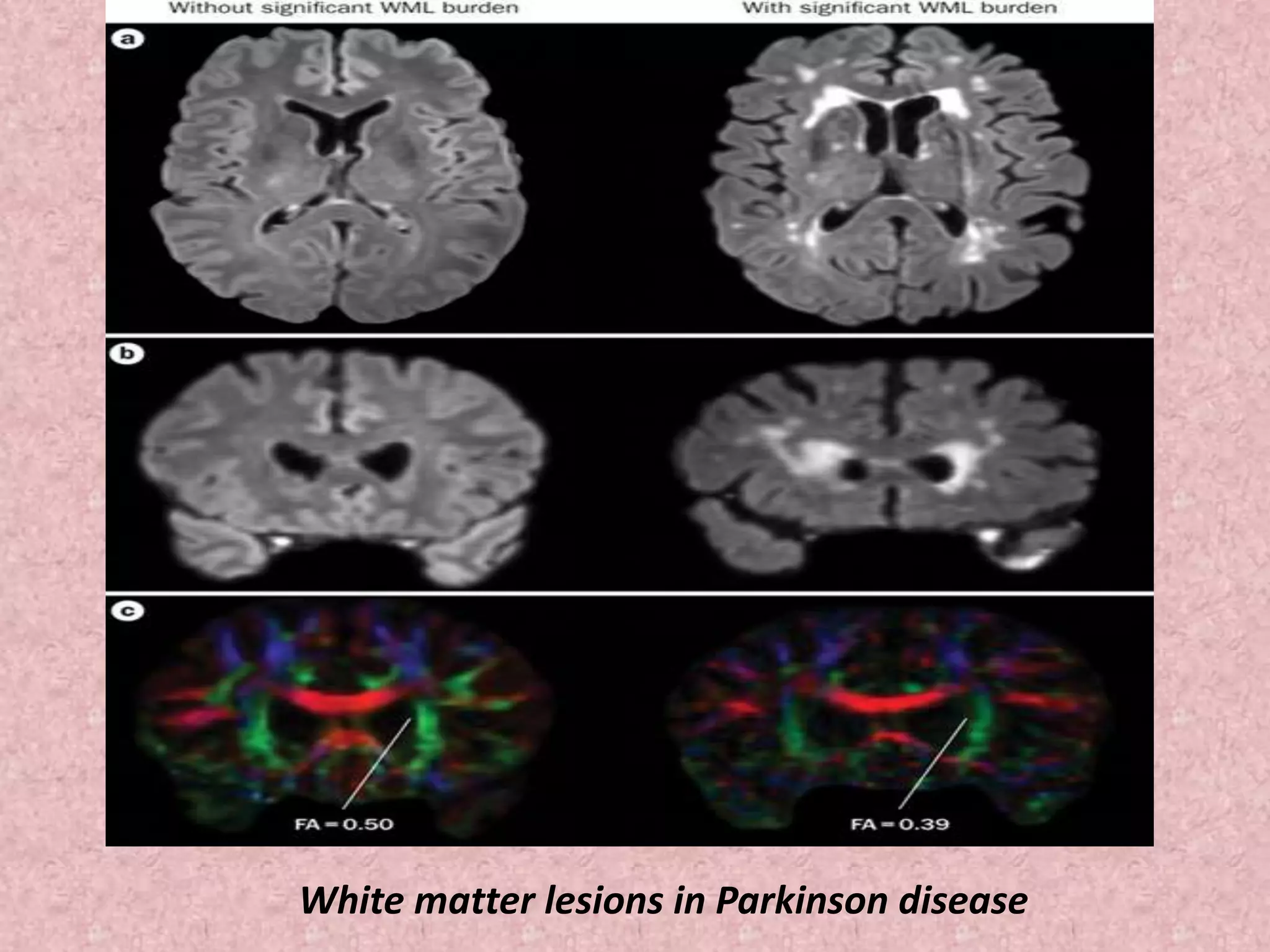
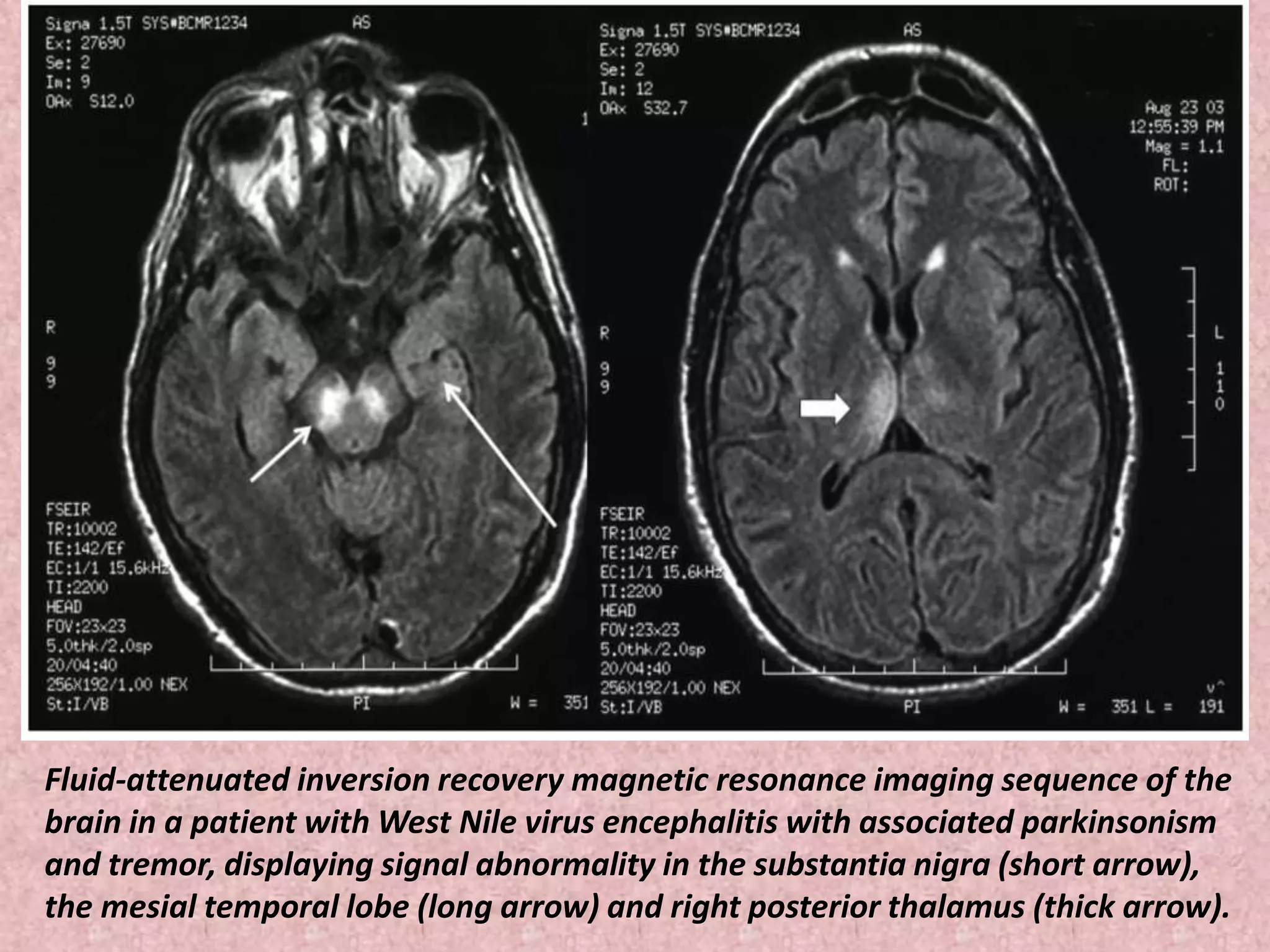
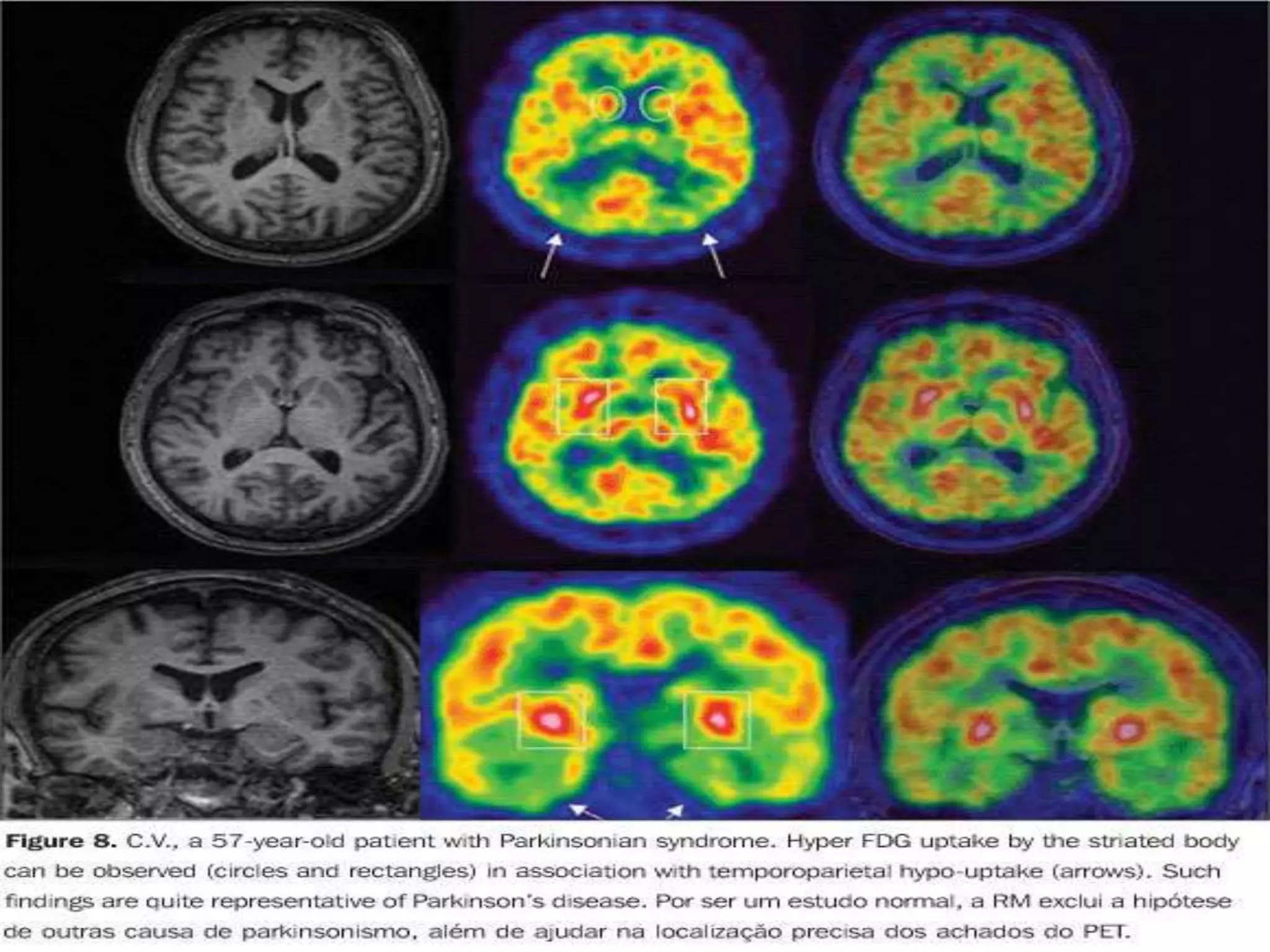
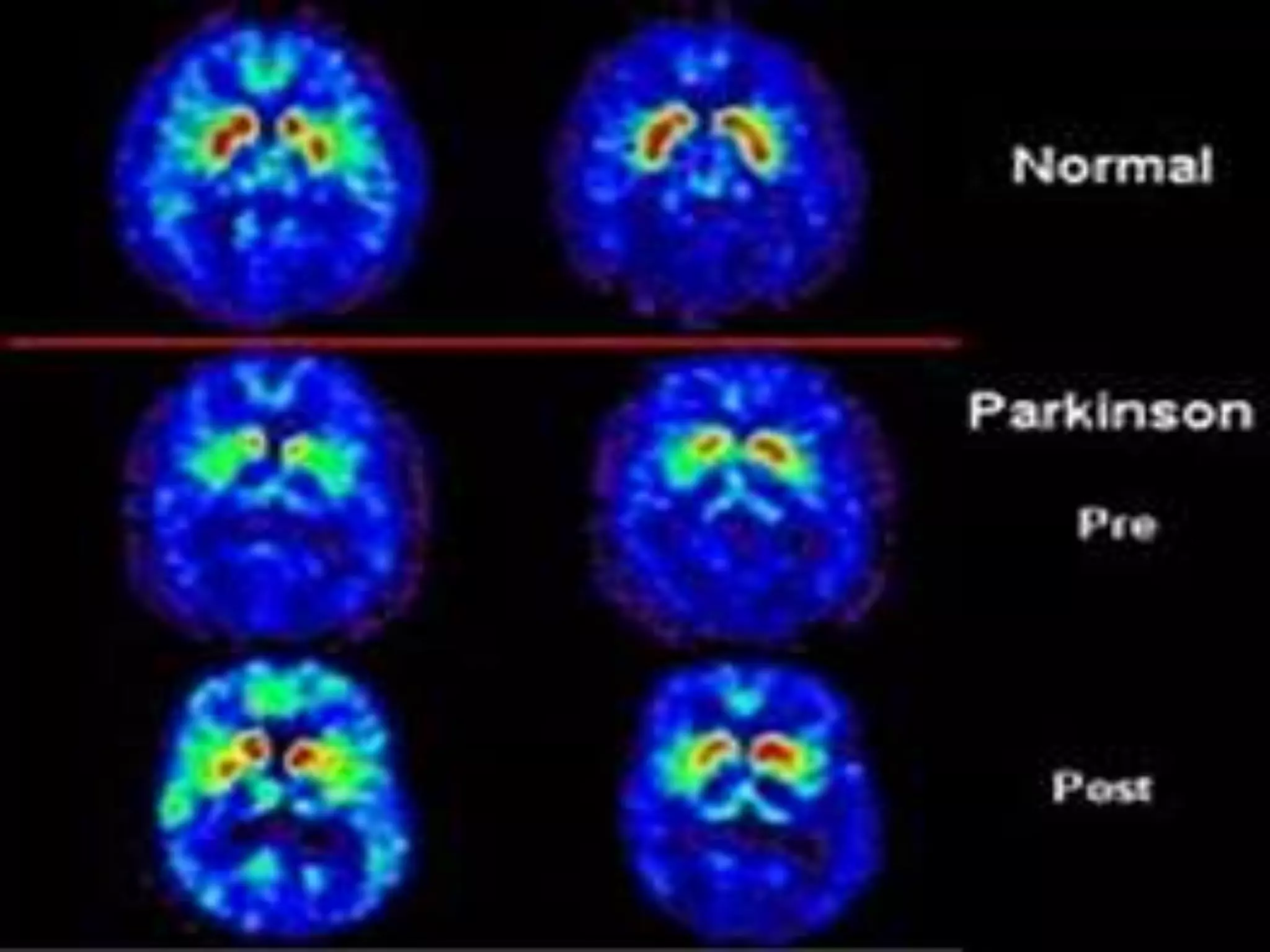
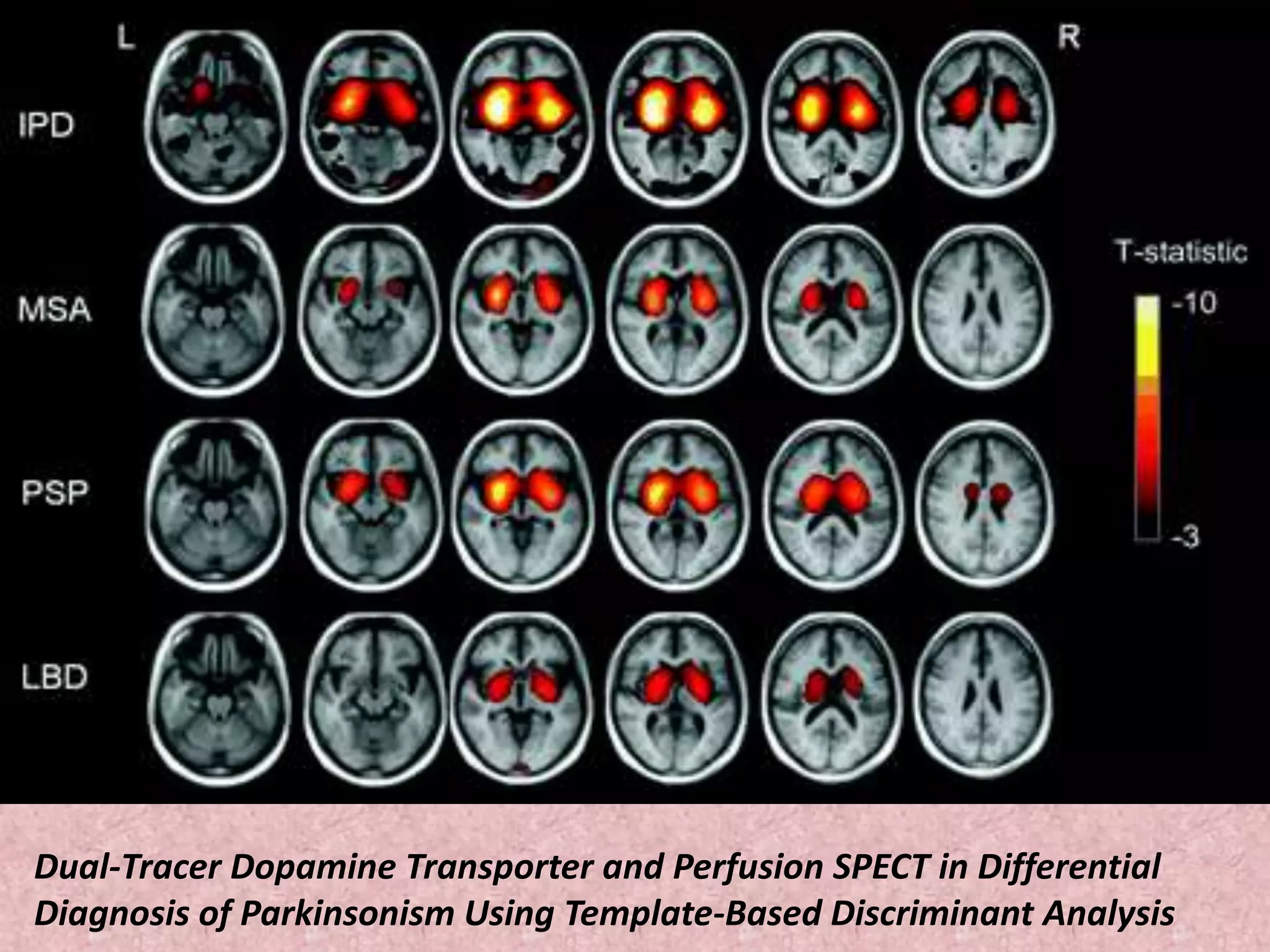
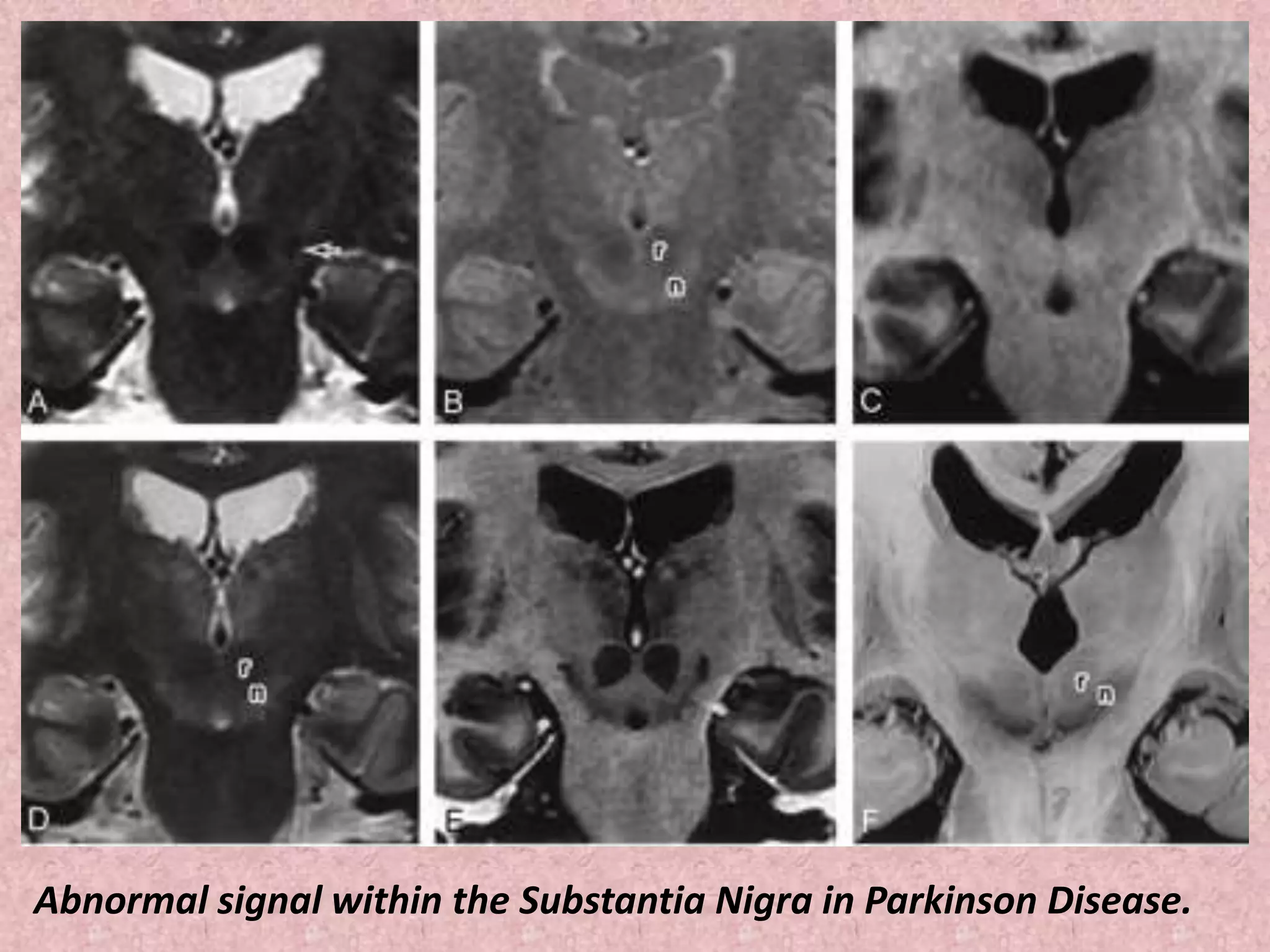
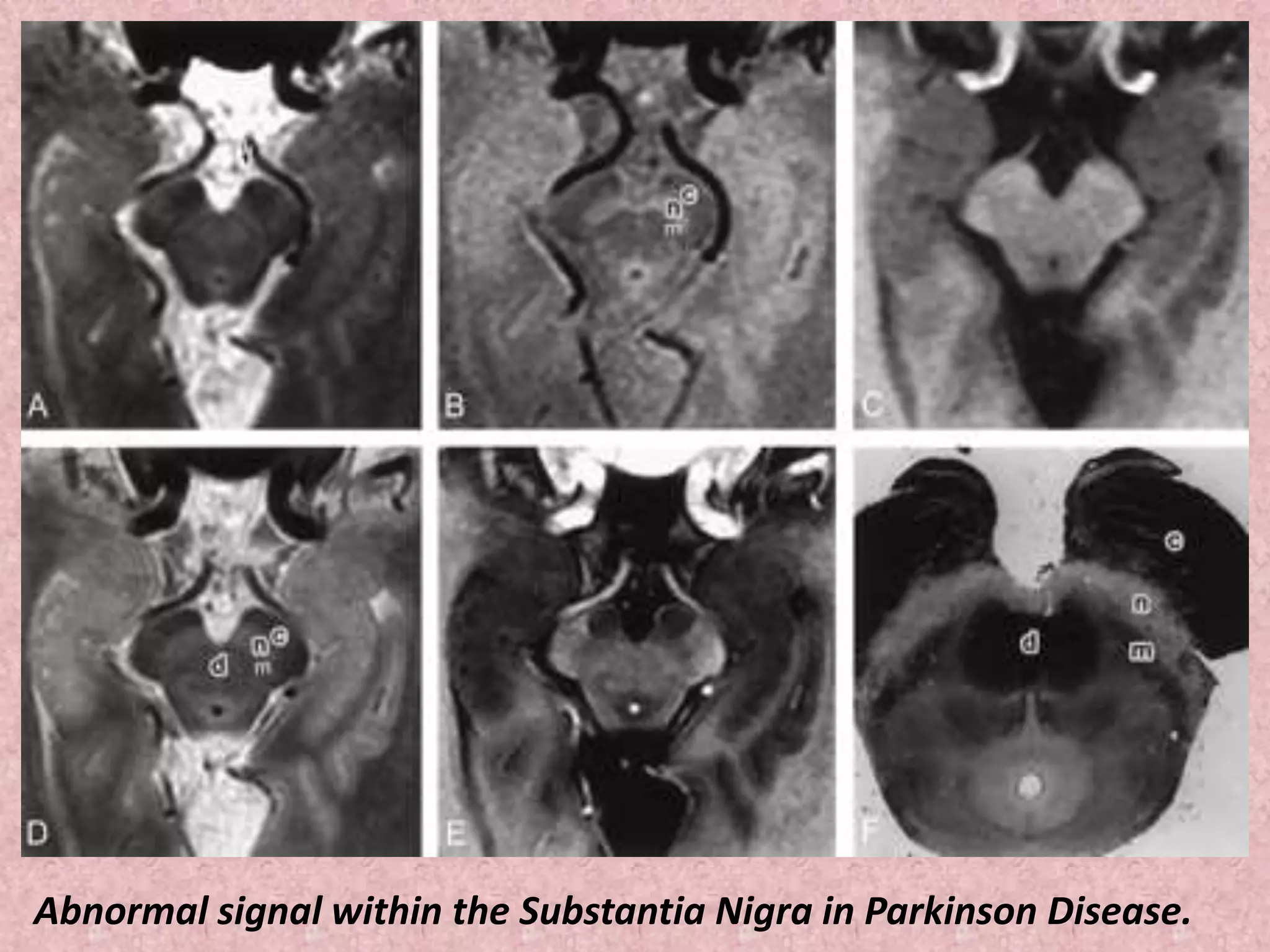
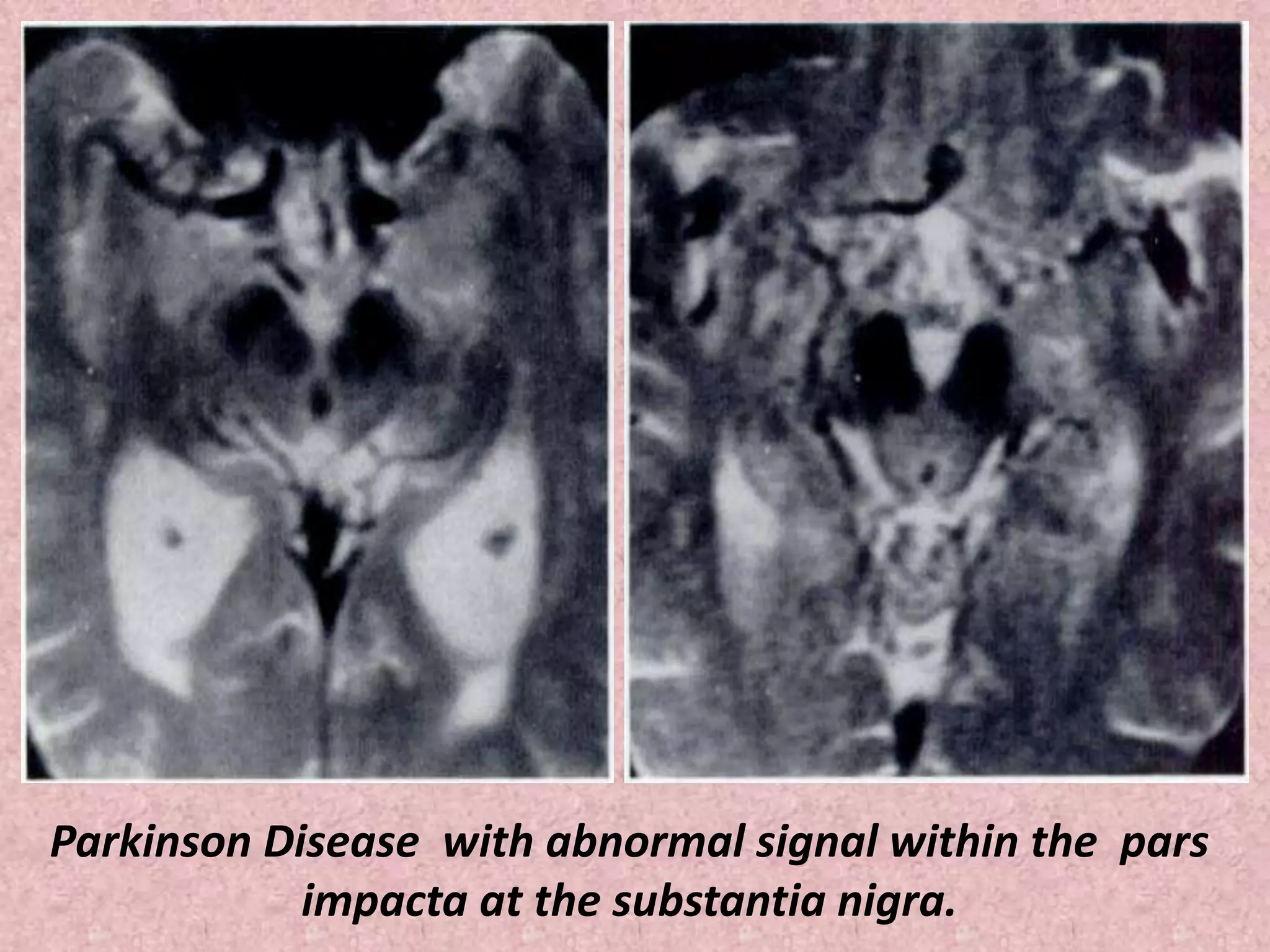
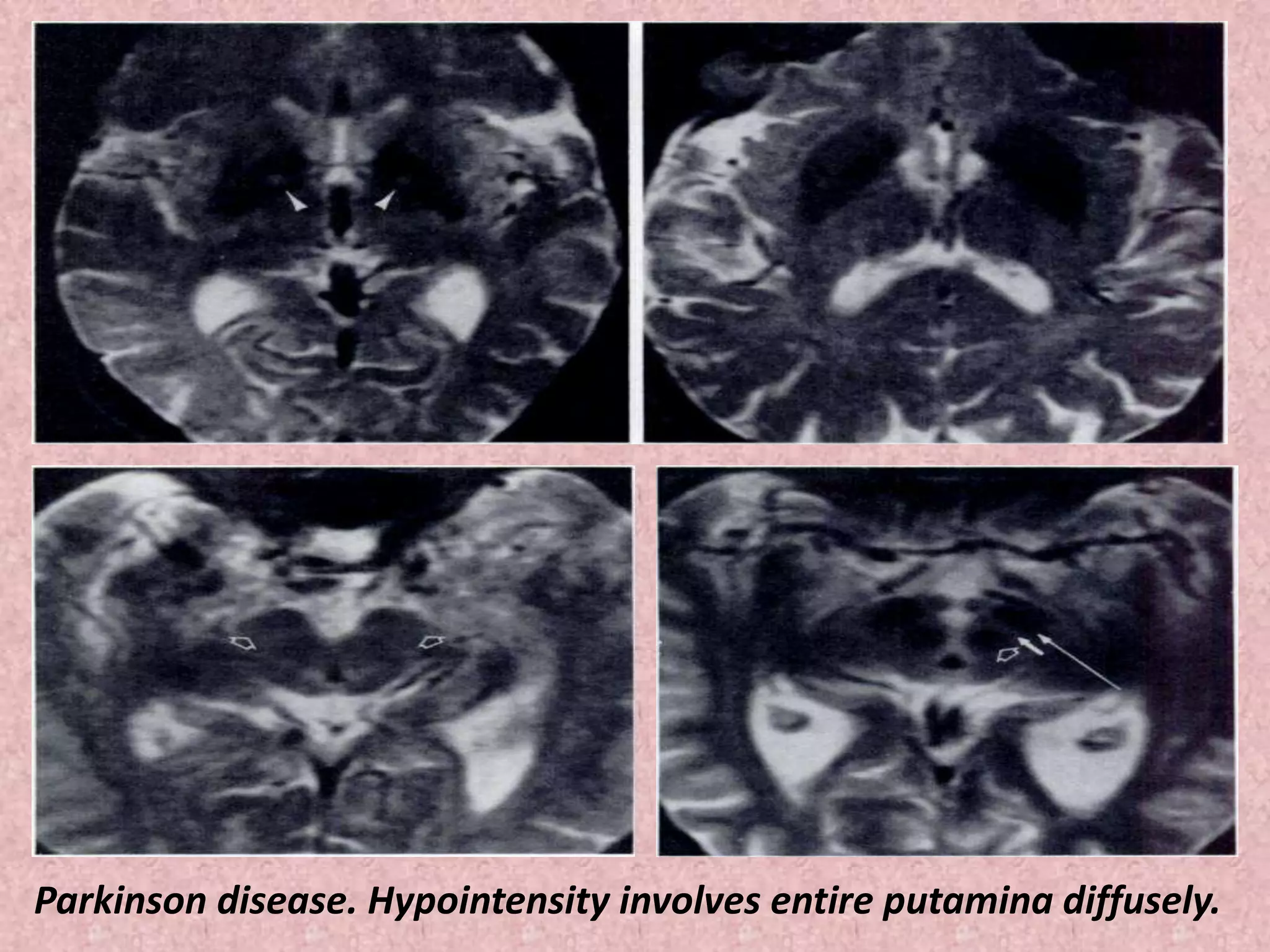
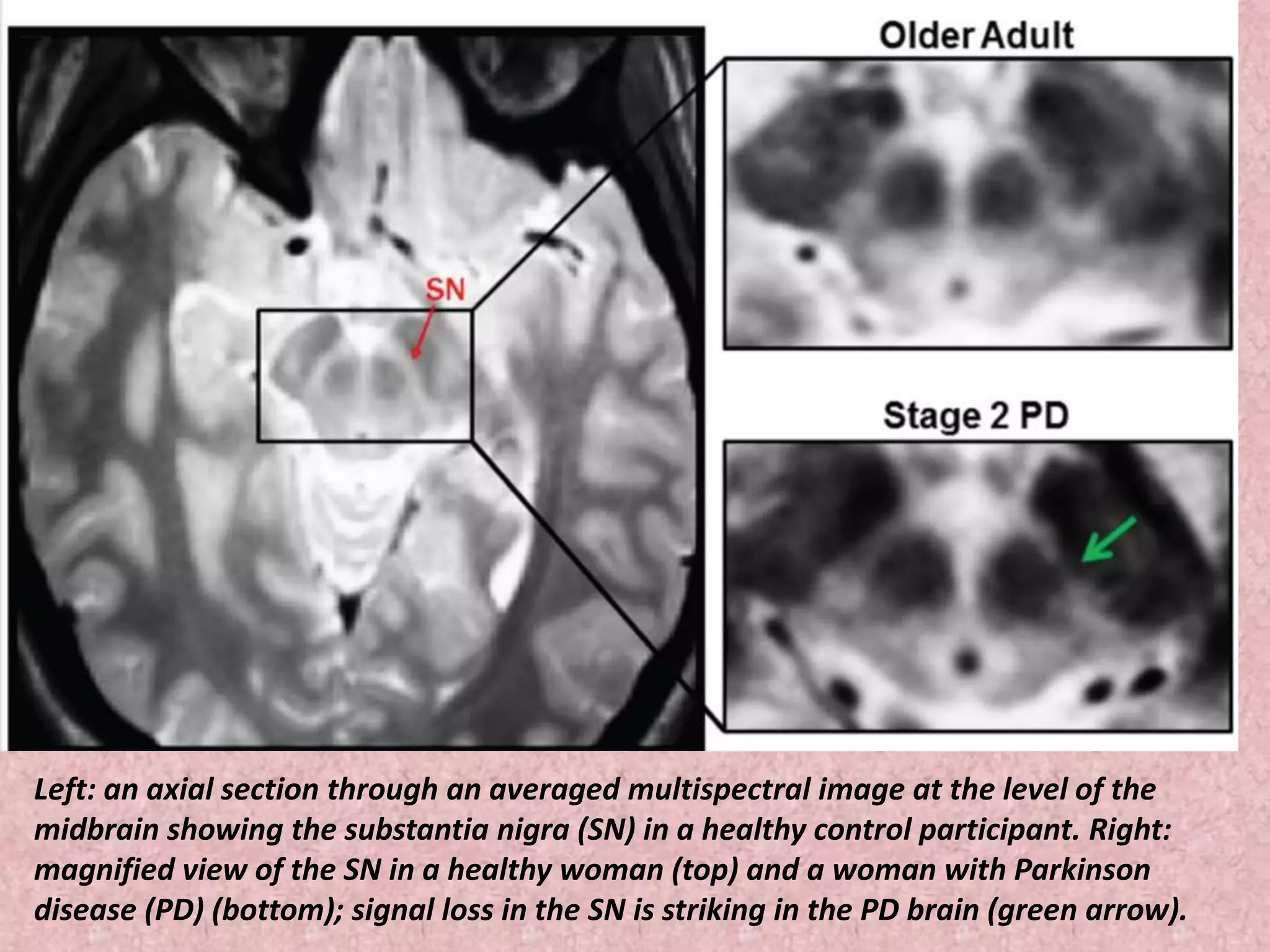
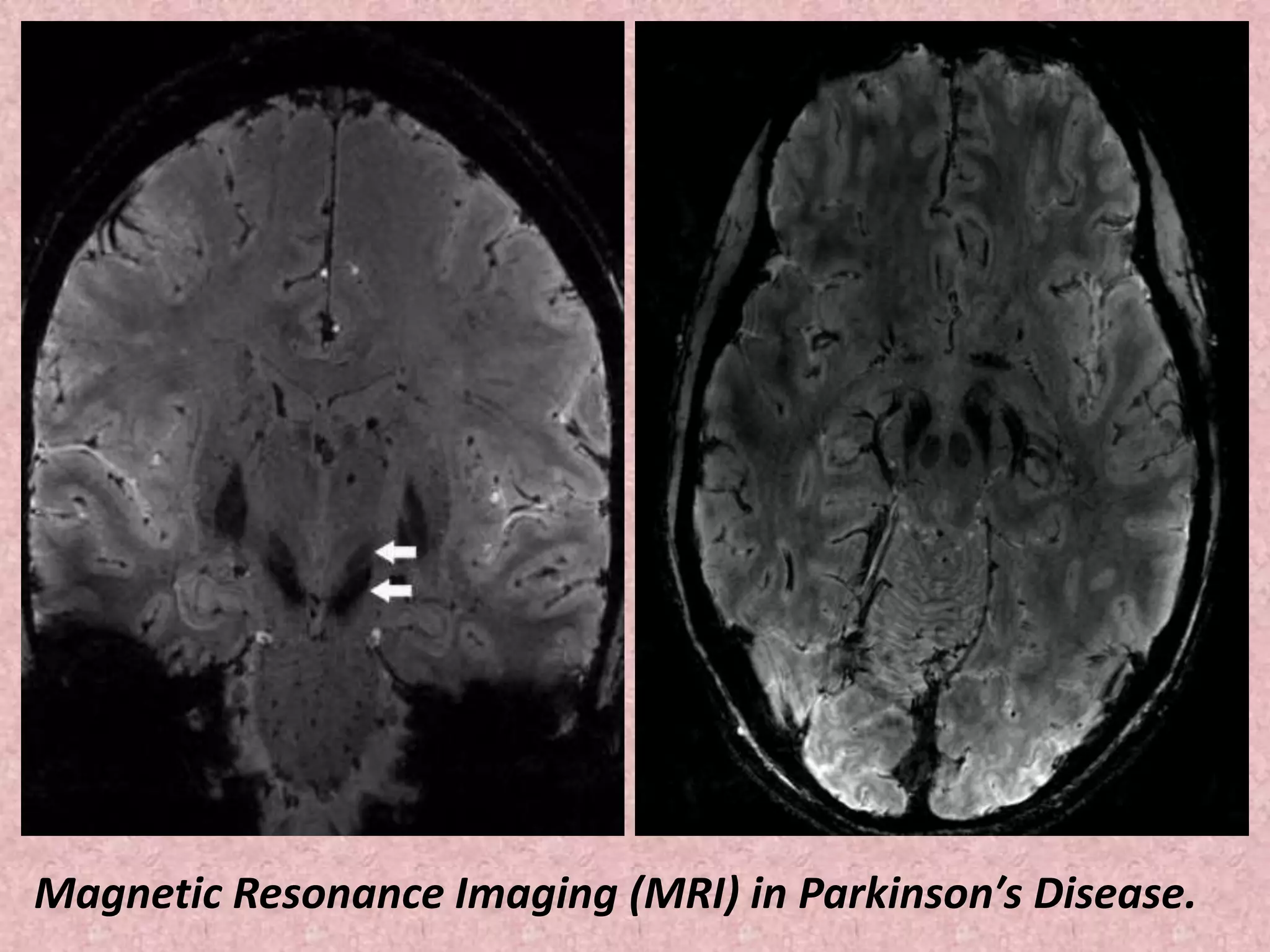
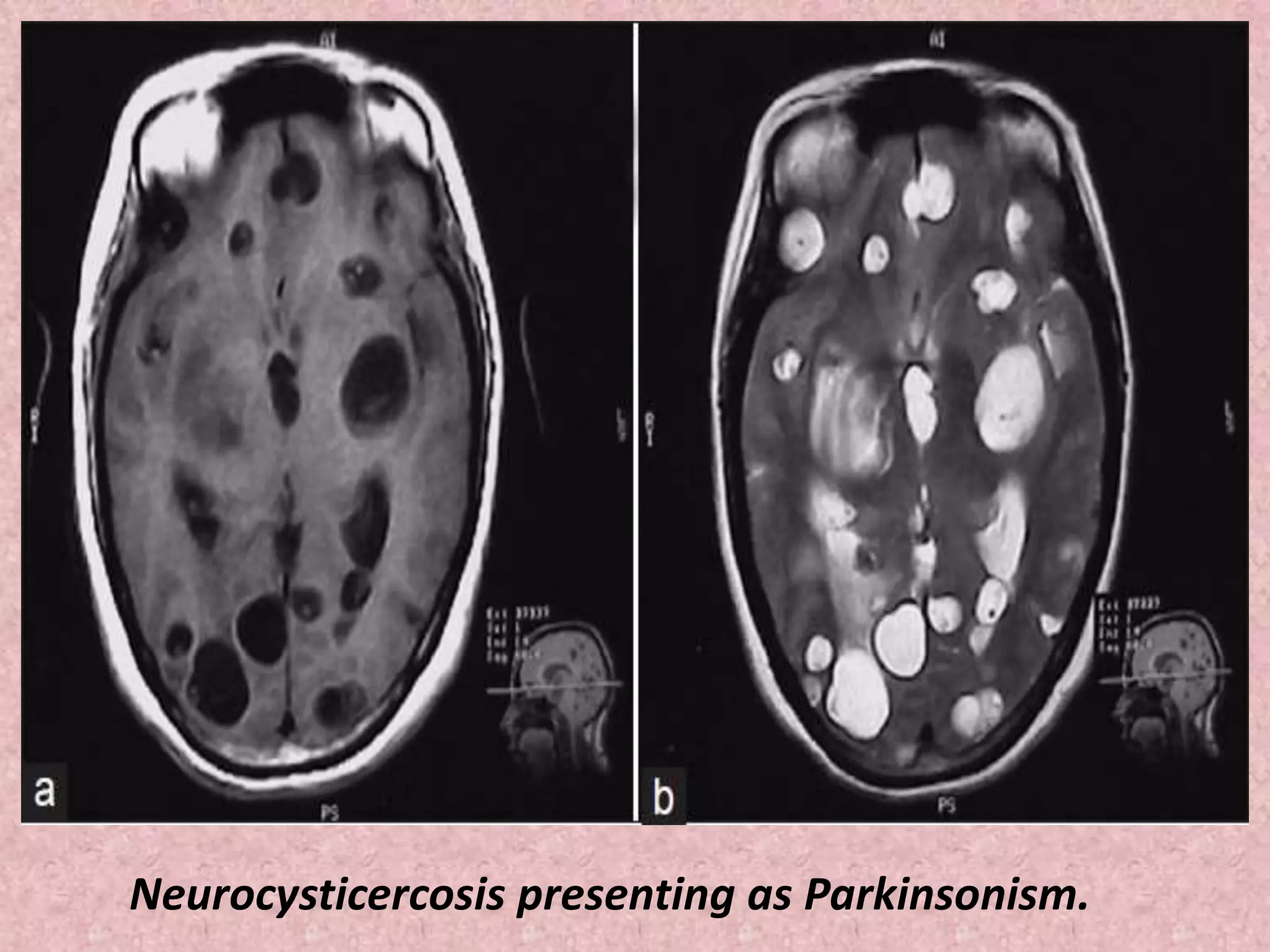

This document discusses Parkinson's disease and parkinsonism. It covers the pathogenesis, classification, clinical features, investigations and imaging findings of Parkinson's disease and other conditions that can cause parkinsonian symptoms. Imaging plays an important role in the diagnosis and differential diagnosis of parkinsonism. Techniques like DAT imaging and MRI can help differentiate Parkinson's disease from other neurodegenerative diseases and conditions.























































































