Downloaded 590 times

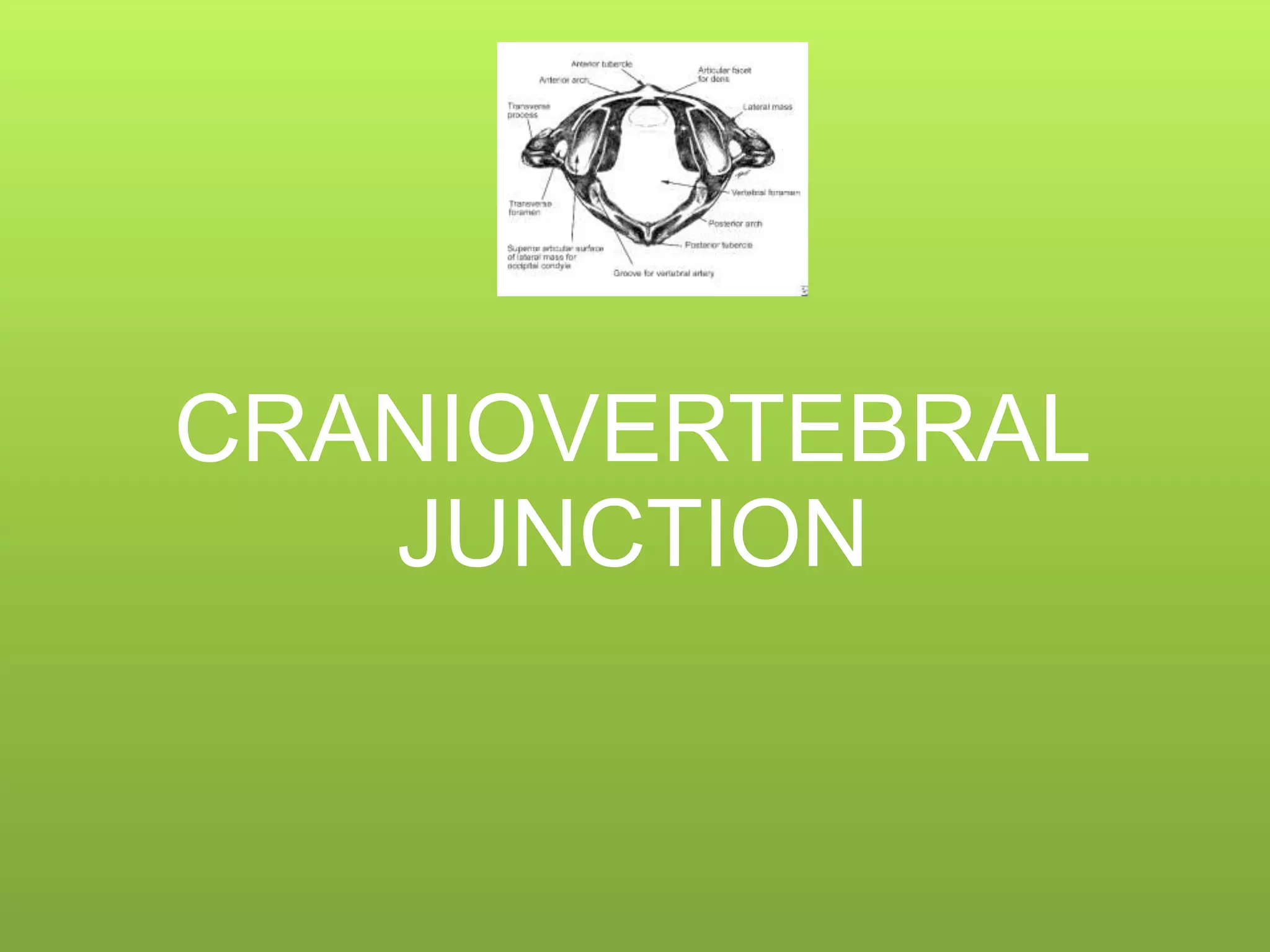
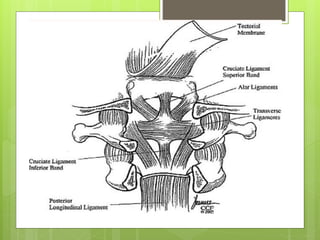
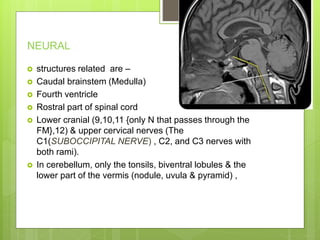

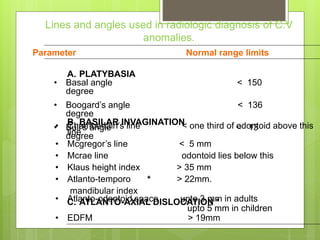
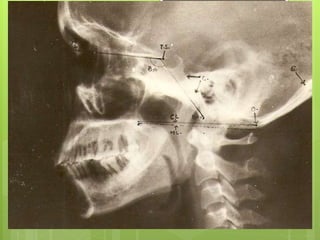


The craniovertebral junction (CVJ) refers to the occiput, atlas, axis, and supporting ligaments. It is a transition zone between the mobile cranium and spinal column. The CVJ encloses important neural and vascular structures. Anatomically, the CVJ includes bony structures like the occiput, atlas, and axis along with their articulations and connecting ligaments. It also has muscles, neural elements like the medulla and lower cranial nerves, lymphatics, arteries and veins. Congenital anomalies of the CVJ can occur due to malformations during embryological development. Radiological evaluation of the CVJ involves measurements and angles on X




















































































