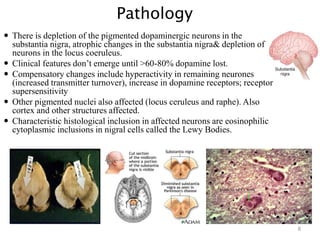

![Investigations:
The diagnosis is made clinically, as there is no diagnostic test for Parkinson's
disease.
Imaging (CT or MRI) of the head may be needed if there are any features
suggestive of pyramidal, cerebellar or autonomic involvement, or the
diagnosis is otherwise in doubt (e.g to exclude stroke).
20
[18F]dopa PET and β-CIT SPECT images.
[18F]dopa PET uptake in the putamen
is reduced in PD.](https://image.slidesharecdn.com/parkinsonsdisease-170221065656/85/Parkinson-s-disease-20-320.jpg)

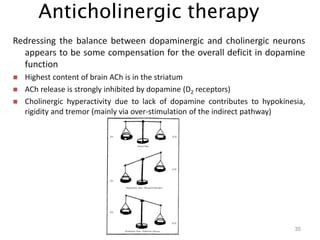

This document provides an overview of Parkinson's disease, including its etiology, incidence, pathophysiology, clinical presentation, diagnosis, prognosis, and treatment. Some key points: - Parkinson's disease is a chronic neurodegenerative disorder that affects the basal ganglia and is characterized by bradykinesia, rigidity, tremor, and postural instability. - It has an annual incidence of 0.2 per 1000 people and prevalence of 1.5 per 1000. Risk increases with age. - Pathologically it involves the loss of dopamine-producing neurons in the substantia nigra and formation of Lewy bodies. - Clinical diagnosis is based on the presence of cardinal motor symptoms
































































































