Downloaded 181 times

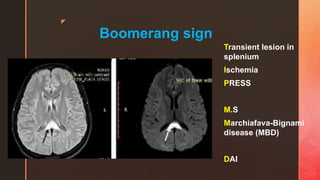

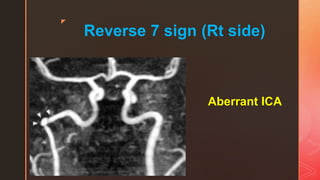









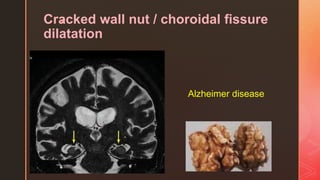


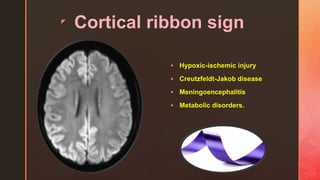
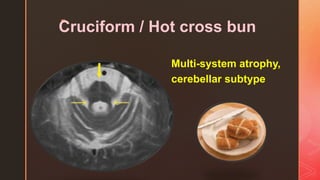



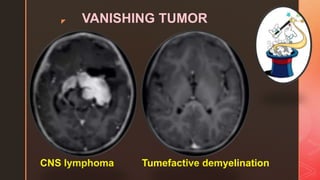


















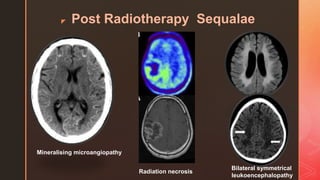
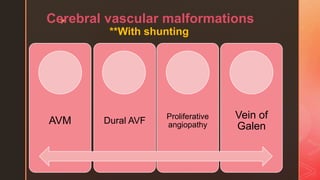


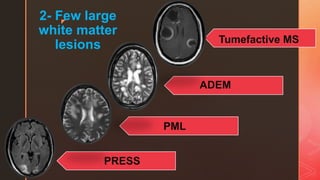
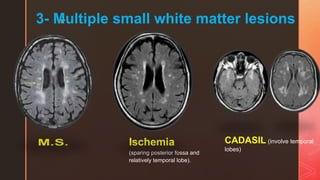















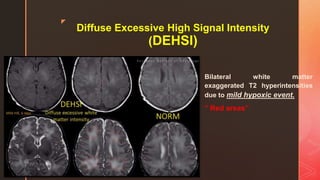


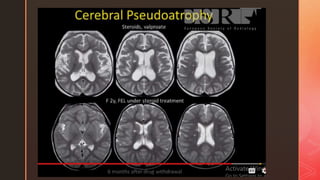
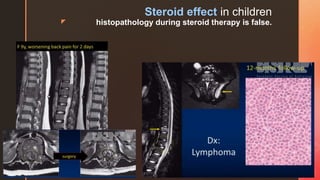








This document provides descriptions and images related to various neuroimaging signs seen in neuroradiology. It discusses signs seen in conditions such as multiple sclerosis, CADASIL, ischemic and hemorrhagic strokes, infections like abscesses, tumors, and other pathologies. Specific signs described include the boomerang sign, butterfly medulla sign, onion rings sign, trident sign, and others. Imaging features of various diseases and abnormalities are also outlined.