Downloaded 79 times

![DISCUSSION
In the last few years, an upward trend has been occurring in the number of female patientsIn the last few years, an upward trend has been occurring in the number of female patients
with post-MI VSD, and increased mortality among these patients.with post-MI VSD, and increased mortality among these patients.
A change in frequency of VSD location has been occurring; in the past, rupture was more likelyA change in frequency of VSD location has been occurring; in the past, rupture was more likely
to involve anterior region of the left anterior descending artery basin, whereas recent datato involve anterior region of the left anterior descending artery basin, whereas recent data
shows predominance in the inferior–posterior region.shows predominance in the inferior–posterior region.
Despite intervention, operative mortality for post-MI VSD repair remains high (from 20% toDespite intervention, operative mortality for post-MI VSD repair remains high (from 20% to
40% by several studies40% by several studies
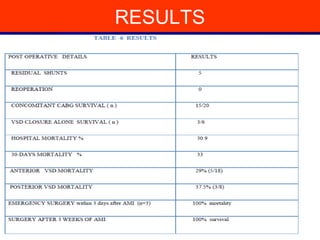
Our 30-day mortality rate was comparable at 33%.Our 30-day mortality rate was comparable at 33%.
Preoperative status of the patient has a bearing on prognosis.Preoperative status of the patient has a bearing on prognosis.
Poor ventricular function , deteriorating cardiovascular status [9], cardiogenic shock[10], inferiorPoor ventricular function , deteriorating cardiovascular status [9], cardiogenic shock[10], inferior
MI [10,11], increasing age ,and inotrope requirements have all been shown to be associatedMI [10,11], increasing age ,and inotrope requirements have all been shown to be associated
with a poor prognosis.with a poor prognosis.](https://image.slidesharecdn.com/postmivsd-140731215631-phpapp01/85/Post-mi-vsd-17-320.jpg)
![DISCUSSION
The development of shock is the most important predictor of survival. Persistence of class IVThe development of shock is the most important predictor of survival. Persistence of class IV
cardiogenic shock inPVSD is associated with 100% mortality [12].cardiogenic shock inPVSD is associated with 100% mortality [12].
These findings are in line with our results concerning emergency operation. Worst results wereThese findings are in line with our results concerning emergency operation. Worst results were
observed in patients with lack of improvement hemodynamic status in spite the useof an IABP.observed in patients with lack of improvement hemodynamic status in spite the useof an IABP.
A longer time between AMI and surgery favoured survival. Time period from AMI to VSDA longer time between AMI and surgery favoured survival. Time period from AMI to VSD
seems to be a significantfactor of survival.seems to be a significantfactor of survival.
It is clear that the higher mortality in patients operated on early is also due to the seriousnessIt is clear that the higher mortality in patients operated on early is also due to the seriousness
of hemodynamic conditions which do not allow any delay in surgical treatment.of hemodynamic conditions which do not allow any delay in surgical treatment.
Higher mortality reported in posterior VSD can either be related to greater technical difficultiesHigher mortality reported in posterior VSD can either be related to greater technical difficulties
associated with surgical repair or to a higher incidence of right ventricular failure [17,18associated with surgical repair or to a higher incidence of right ventricular failure [17,18
Chronic VSD is easier to repair since the septum is well scarred and the patch can be securelyChronic VSD is easier to repair since the septum is well scarred and the patch can be securely
sutured .sutured .](https://image.slidesharecdn.com/postmivsd-140731215631-phpapp01/85/Post-mi-vsd-18-320.jpg)



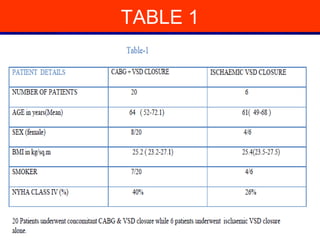
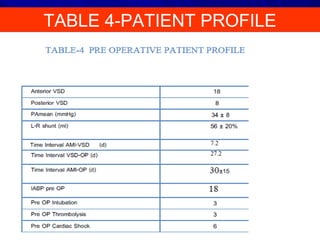
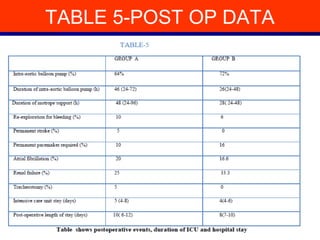
This study evaluated outcomes of 26 patients who underwent surgical repair of post-myocardial infarction ventricular septal defect (VSD) at Nizams Institute of Medical Sciences between 1997-2012. 20 patients underwent VSD repair with concomitant coronary artery bypass grafting, while 6 had VSD closure alone. The mean time between MI and VSD appearance was 7.2 days, and between VSD appearance and surgery was 27.2 days. Overall in-hospital mortality was 30.9% and 30-day mortality was 33%. Patients who underwent emergency surgery within 3 days of MI had 100% mortality, while those operated on after 3 weeks had 100% survival. Concomitant CABG during VSD repair was associated with lower
































































































