Downloaded 410 times
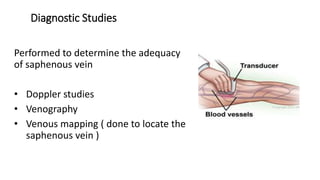
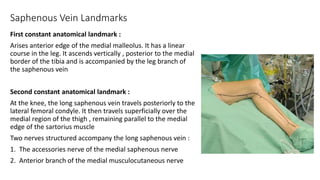
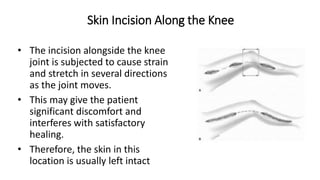
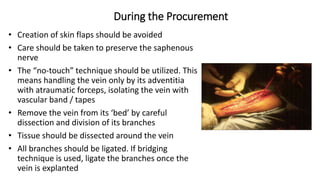
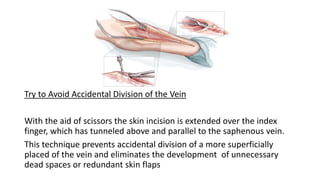
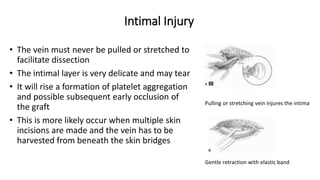
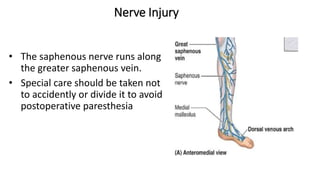

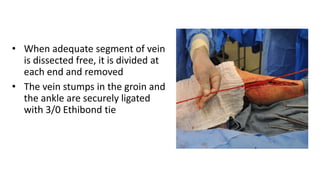
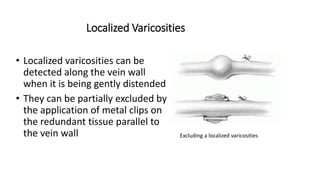
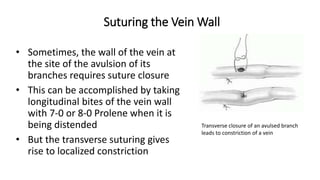




This document discusses saphenous vein harvesting for coronary artery bypass grafting (CABG). It covers the anatomy of the saphenous vein, techniques for harvesting including open and endoscopic methods, tips for avoiding complications, and postoperative care. The saphenous vein is commonly used as a graft due to its accessibility and handling properties, though the internal mammary artery is preferred due to better long-term patency rates. Care must be taken during harvesting to avoid intimal injury, nerve damage, and ensure hemostasis and wound closure to prevent infection.




![ESVS Guidelines ALI 2020 - MARGA compressed [Repaired].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/esvsguidelinesali2020-margacompressedrepaired-221116034136-273c0e6d-thumbnail.jpg?width=640&height=640&fit=bounds)






























































