Downloaded 491 times




















![PROMOTIONALAND MOTIVATIONAL
MEASURES FOR ADOPTION OF THE SMALL
FAMILY NORM:
• A Family Welfare linked Health Insurance plan. – for acceptors
and indemnity cover(Rs 2 lac) for doctors in accredited facilities.
Compensation Death : < 7 days (Rs 2 lac), 8-30 (Rs 50,000), <60
days (Rs 25,000) in Failure (Rs 30,000)
• All India Hospital postpartum programme (AIHPP)
• Cash Incentives – for acceptors- tubectomy [Rs 600, 145(lap)],
vasectomy (Rs 1100), IUD (Rs 75). For motivators – tubectomy (Rs
150), vasectomy (Rs 200).
• State/ central govt. Employees get special increments after
sterilization with special leaves.](https://image.slidesharecdn.com/populationfinal-150114081848-conversion-gate01/85/Population-Explosion-in-India-49-320.jpg)








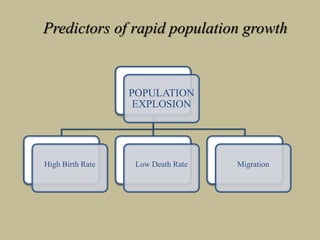
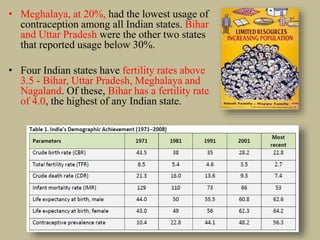
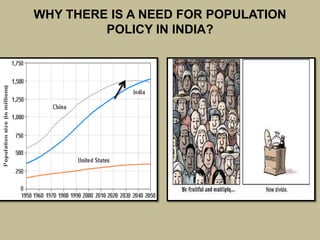
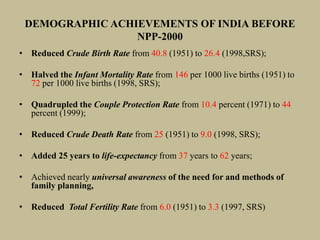
The document discusses India's population growth and the government's strategies to address it. It notes that India has a high population growth rate due to high birth rates and declining death rates. The government has implemented several programs to promote family planning like the National Population Policy 2000 and Janani Suraksha Yojana. However, challenges remain as many states still have high total fertility rates and low contraceptive use. The government is working to improve access to and use of family planning services through integrated healthcare programs and effective communication initiatives.