Downloaded 3,215 times





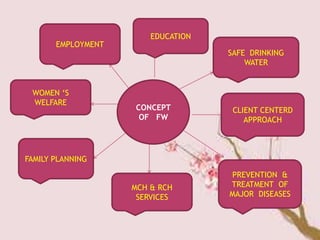

























The National Family Welfare Programme was launched in 1952 in India to promote family planning. It aims to improve quality of life through various components like administration, training, health education, and family planning services. The Reproductive and Child Health Programme was launched in 1997 to further the objectives of reducing infant and maternal mortality rates. It provides maternal and child healthcare services, family planning, and prevention of HIV/AIDS. The various methods of family planning discussed are natural methods, mechanical methods, hormonal methods, and surgical methods.