Download as PDF, PPTX

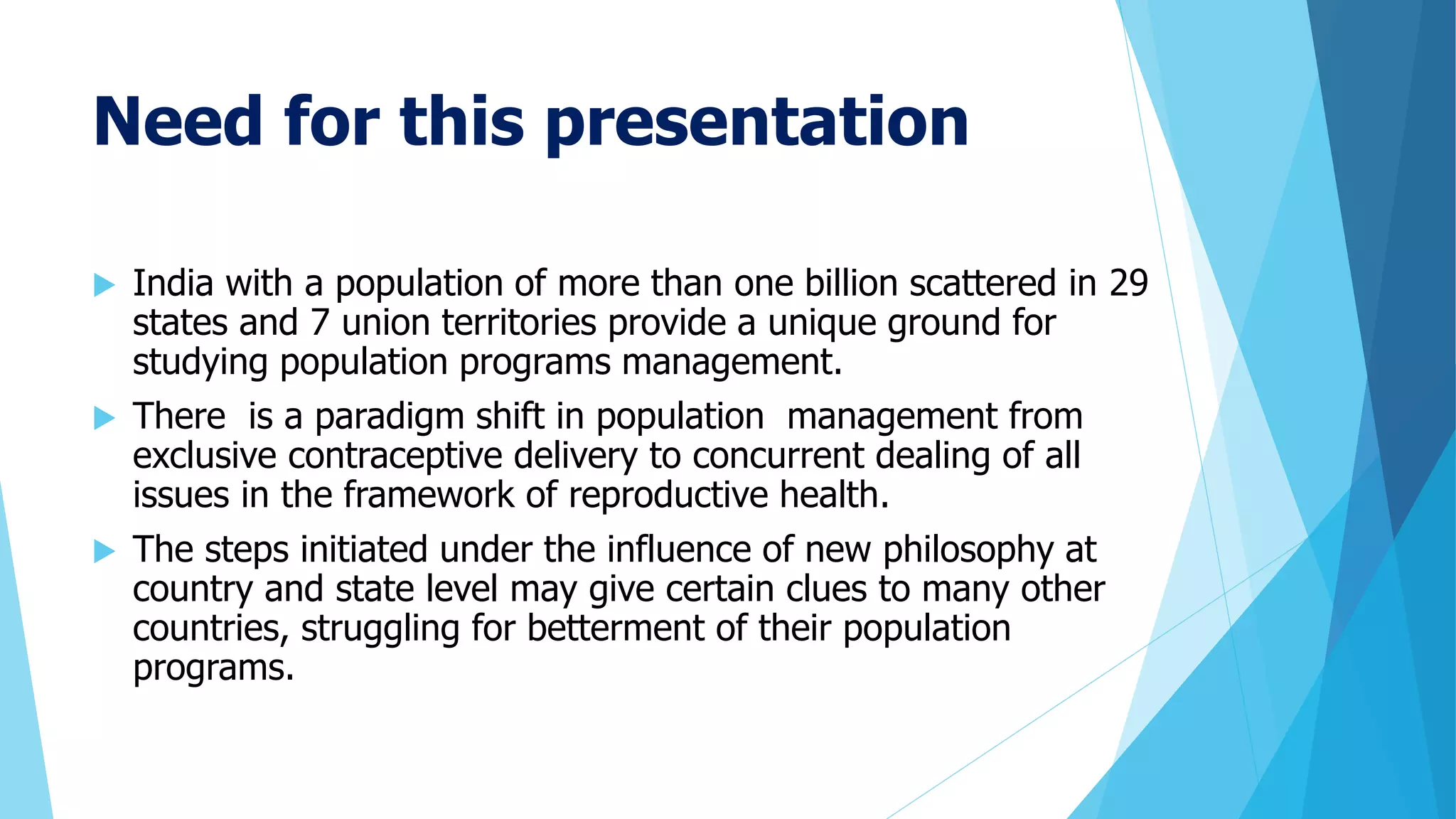
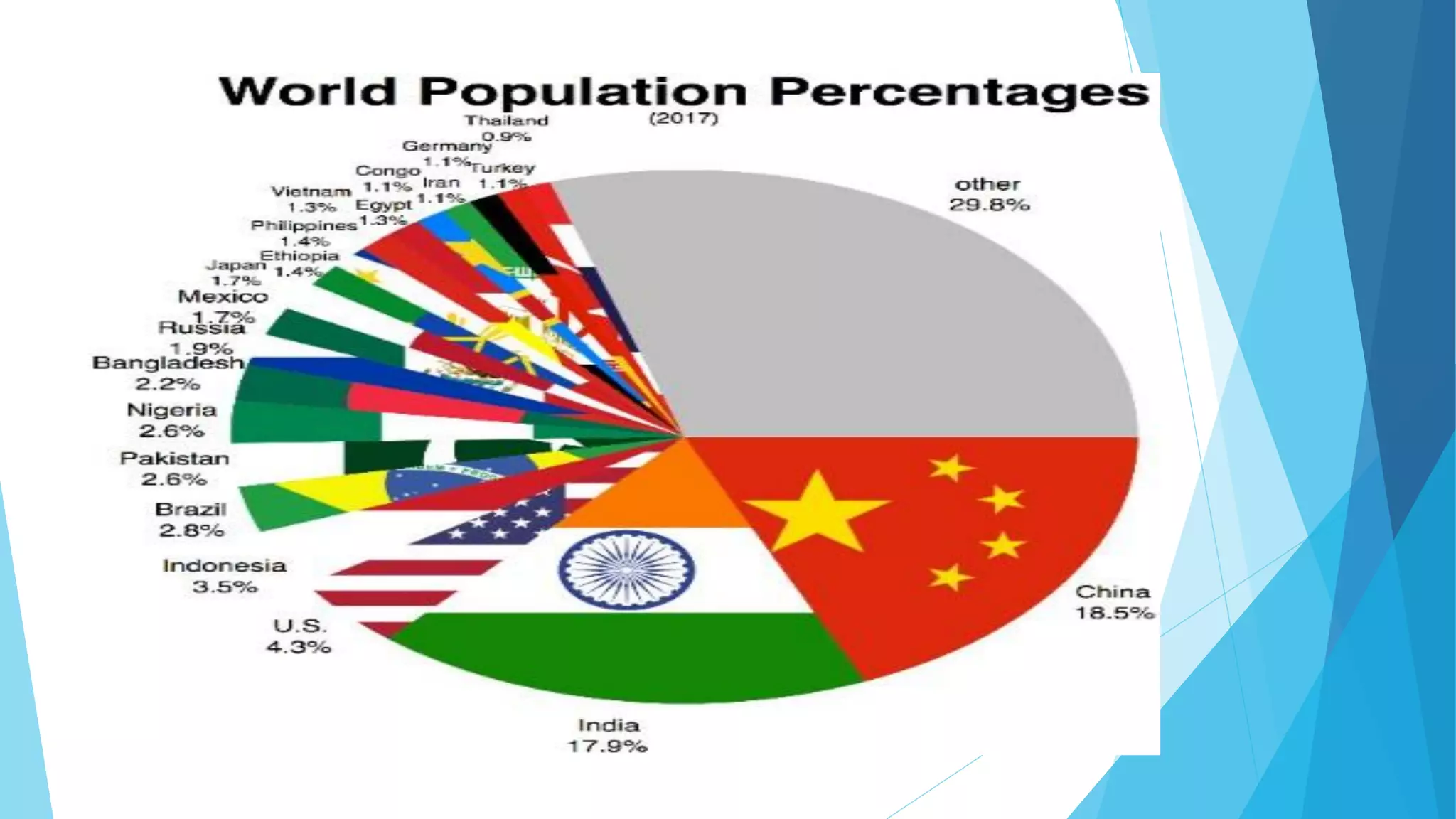






























































The document summarizes India's national population policy and programs. It discusses the need for a population policy given India's large population size. It outlines the key objectives and strategies of national population policies over time, including increasing the legal age of marriage, promoting birth control methods, and integrating population concerns into five-year economic plans. The national population policy aims to stabilize population growth and achieve a level consistent with sustainable development.