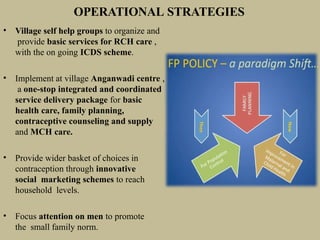
The document discusses the population explosion in India, highlighting the current status, causes, and the government's strategies to address the issue. It outlines the challenges posed by rapid population growth, including social, economic, and environmental impacts, as well as the need for effective family planning and policy measures. The National Population Policy of 2000 aims to stabilize population growth in a sustainable manner through various initiatives and objectives focused on health care, education, and service accessibility.





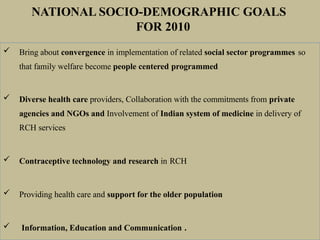
![PROMOTIONAL AND MOTIVATIONAL
MEASURES FOR ADOPTION OF THE SMALL
FAMILY NORM:
• A Family Welfare linked Health Insurance plan. – for acceptors
and indemnity cover(Rs 2 lac) for doctors in accredited facilities.
Compensation Death : < 7 days (Rs 2 lac), 8-30 (Rs 50,000),
<60 days (Rs 25,000) in Failure (Rs 30,000)
• All India Hospital postpartum programme (AIHPP)
• Cash Incentives – for acceptors- tubectomy [Rs 600, 145(lap)],
vasectomy (Rs 1100), IUD (Rs 75). For motivators – tubectomy
(Rs 150), vasectomy (Rs 200).
• State/ central govt. Employees get special increments
after sterilization with special leaves.](https://image.slidesharecdn.com/population-250103151210-2cd64528/85/population-POWERPOINT-PRESENTATION-IN-SOCIOLOGY-42-320.jpg)