1. The document describes how to test various superficial and deep reflexes through elicitation techniques and provides clinical significance of reflex assessment.
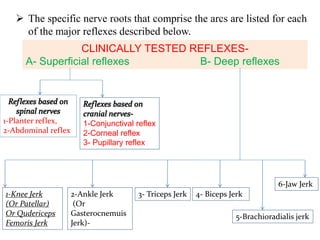
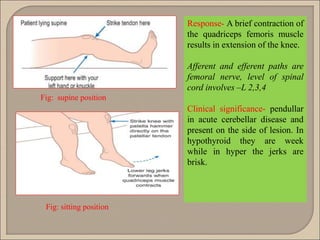
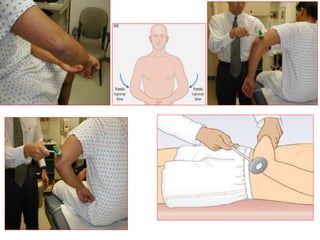
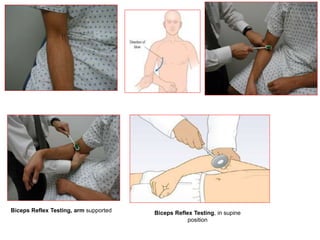
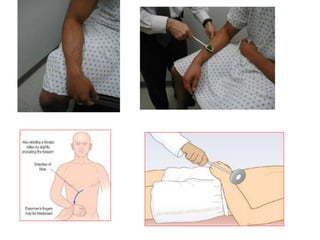
2. Superficial reflexes include plantar, abdominal, and cranial nerve reflexes while deep reflexes tested are knee jerk, ankle jerk, biceps, triceps, and brachioradialis jerks.
3. Abnormal reflexes can indicate lesions in the sensory, motor or central pathways and provide clues to neurological conditions like diabetes, thyroid disorders, or spinal cord injuries. Precise diagnosis requires correlating reflex findings with the clinical picture.