This document discusses phimosis and circumcision. It provides background information on phimosis including definitions, types, epidemiology, embryology, anatomy, etiology, pathophysiology, prognosis, history and physical examination. It also discusses the medical and surgical treatment of phimosis, including conservative surgical alternatives and conventional male circumcision. The document is authored by multiple professors and assistant professors from the Department of Urology at Govt Royapettah Hospital and Kilpauk Medical College in Chennai, India.
![Epidemiology
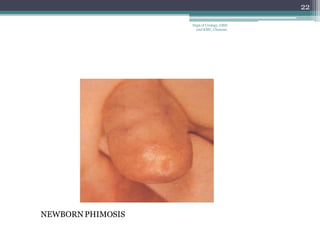
• Nearly all males are born with physiologic phimosis.
• Data have shown that the foreskin is retractable in
90% of boys by age 3 years.
• Only 1% of boys have physiologic phimosis that
persists until age 17 years.
• Thus, most healthy adult men should not have
phimosis; the presence of the disorder in an adult
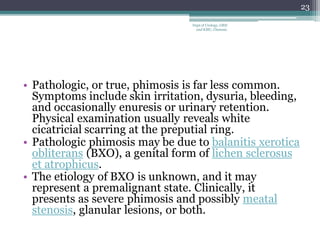
male should raise the suspicion of balanitis
(infection of the foreskin), balanoposthitis (infection
of glans and foreskin), diabetes, [29] or malignancy.
5
Dept of Urology, GRH
and KMC, Chennai.](https://image.slidesharecdn.com/penis-phimosiscircumcision-210610131148/85/Penis-phimosis-amp-circumcision-5-320.jpg)

![Phimosis
• Physical examination usually reveals white
cicatricial scarring at the preputial ring.
Meuli et al devised the following scoring system
to rate the severity of phimosis: [32]
• Grade I - Fully retractable prepuce with stenotic ring
in the shaft
• Grade II - Partial retractability with partial exposure
of the glans
• Grade III - Partial retractability with exposure of the
meatus only
• Grade IV - No retractability
26
Dept of Urology, GRH
and KMC, Chennai.](https://image.slidesharecdn.com/penis-phimosiscircumcision-210610131148/85/Penis-phimosis-amp-circumcision-26-320.jpg)
![Medical Care
• Applications of steroid creams
(0.05% betamethasone) have been used to
manage phimosis medically. [33] The usual
regimen is application of the steroid cream once
or twice daily for 4-6 weeks. Studies have shown
a success rate of 87% with this treatment.
• Higher rates of success have been reported with
concomitant preputial stretching exercises.
29
Dept of Urology, GRH
and KMC, Chennai.](https://image.slidesharecdn.com/penis-phimosiscircumcision-210610131148/85/Penis-phimosis-amp-circumcision-29-320.jpg)