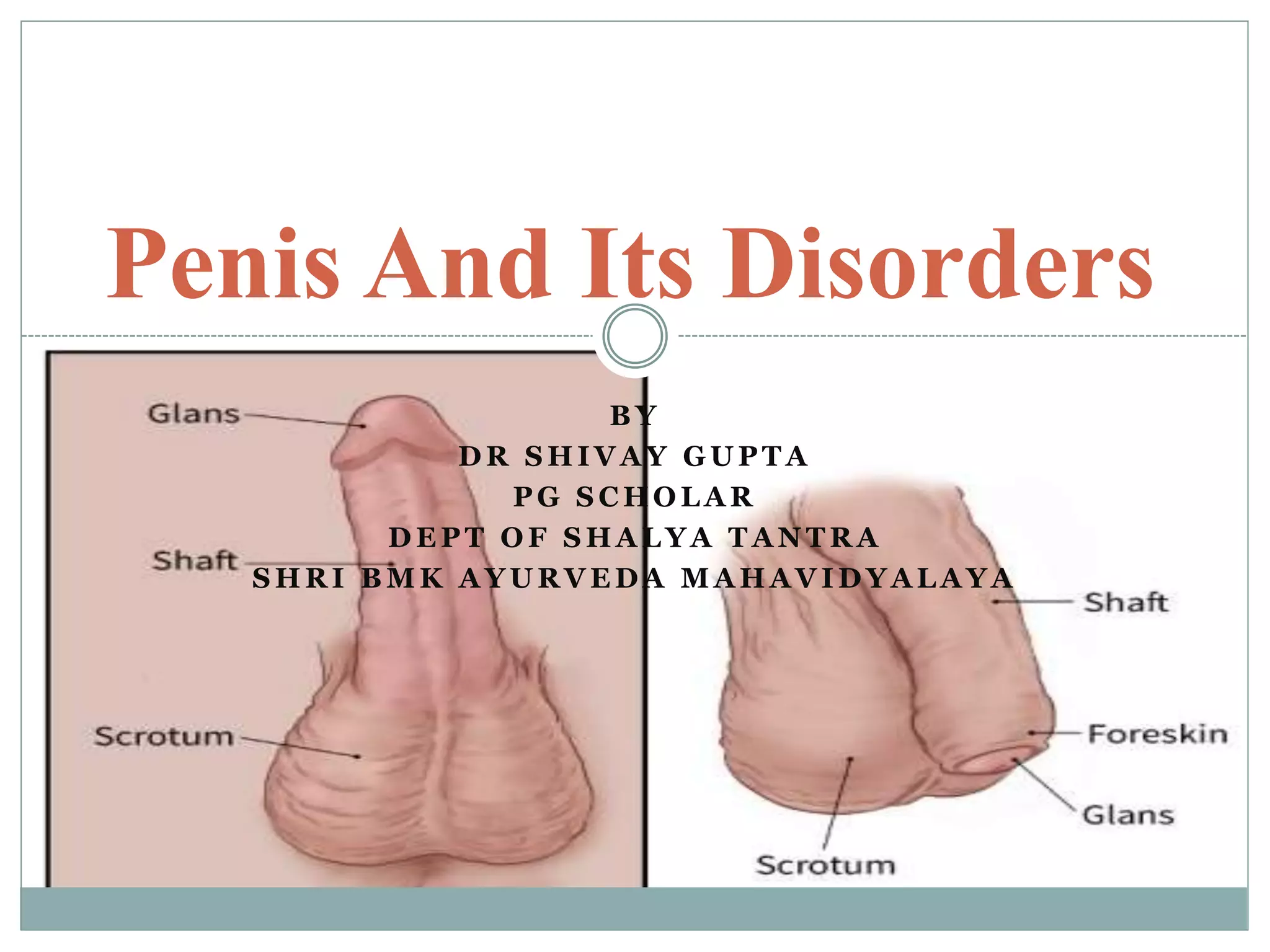
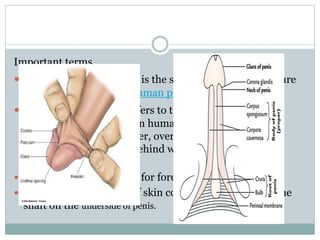
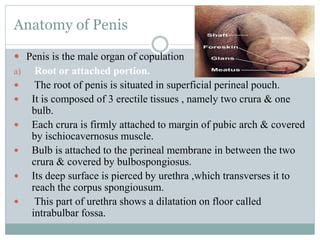
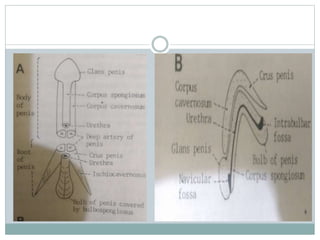
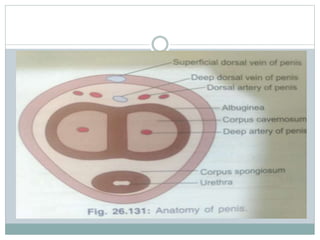
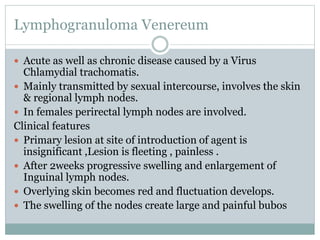
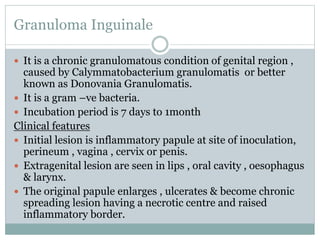
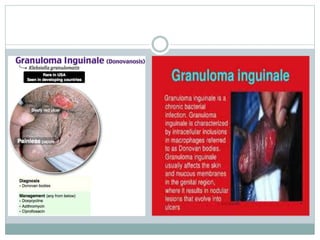
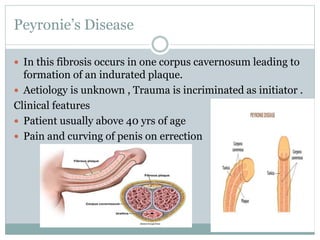
1. The document discusses the anatomy and common disorders of the penis. It describes the structures of the penis including the glans, foreskin, and erectile tissues.
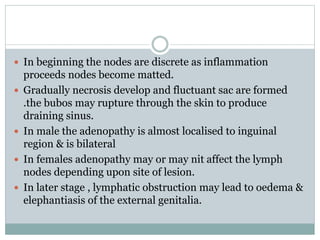
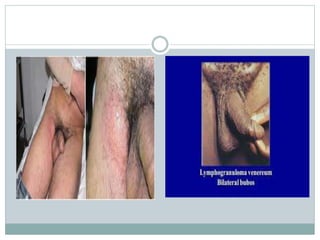
2. Common congenital disorders like hypospadias and epispadias are summarized, as well as acquired conditions such as phimosis, paraphimosis, and lymphogranuloma venereum.
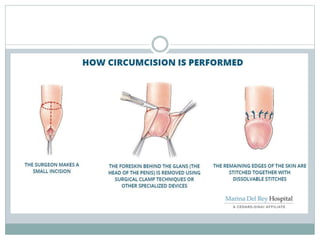
3. Treatment options for these disorders include circumcision to treat phimosis and incision or drainage to treat paraphimosis. Surgery is often used to correct congenital anomalies.



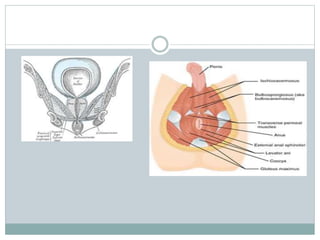
![ The superficial perineal pouch (also superficial perineal
compartment/space/sac) is a compartment of the perineum.
Structure[edit]
The superficial perineal pouch is an open compartment, due to
the fact that anteriorly, the space communicates freely with the
potential space lying between the superficial fascia of the
anterior abdominal wall and the anterior abdominal muscles:
its inferior border is the fascia of Colles, the deeper membranous
layer of the superficial perineal fascia that covers the inferior
border of the muscles of the superficial perineal pouch.
(The fascia of perineum is a deep fascia that covers the
superficial perineal muscles individually).
its superior border is the perineal membrane (inferior fascia of
the urogenital diaphragm).](https://image.slidesharecdn.com/penisdisorders-190123063136/85/Penis-amp-disorders-52-320.jpg)
![ Contents[1][edit]
Muscles
Ischiocavernosus muscle
Bulbospongiosus muscle
Superficial transverse perineal muscle
Erectile bodies
Corpus cavernosum (of penis and of clitoris)
Corpus spongiosus (of penis)
Vessels
Posterior scrotal arteries (males)/Labial arteries (females)
Artery to bulb (males)/vestibule (females)
Urethral artery
Nerves
Posterior scrotal nerves (males)/Posterior Labial nerves(females)
Other
Crura of penis (males) / Crura of clitoris (females)
Bulb of penis (males) / Bulb of vestibule (females)
Bartholin's glands (female)](https://image.slidesharecdn.com/penisdisorders-190123063136/85/Penis-amp-disorders-53-320.jpg)