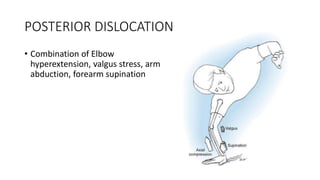
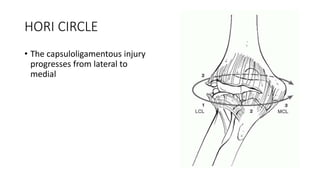
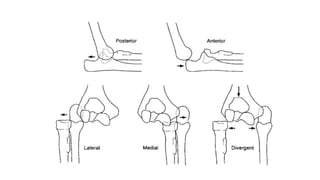
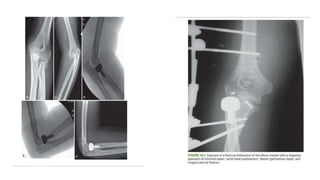
1) Elbow dislocations are most commonly posterior dislocations, which occur due to a combination of hyperextension, valgus stress, arm abduction, and forearm supination.
2) Treatment depends on whether the dislocation is simple or complex, with associated fractures or ligament injuries requiring operative management like open reduction and repair of soft tissues.
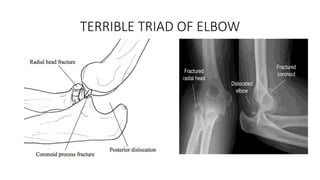
3) The terrible triad of elbow injuries involves a dislocation with fractures of the radial head and coronoid process, requiring restoration of stability through fixation of the fractures and repair of collateral ligaments.