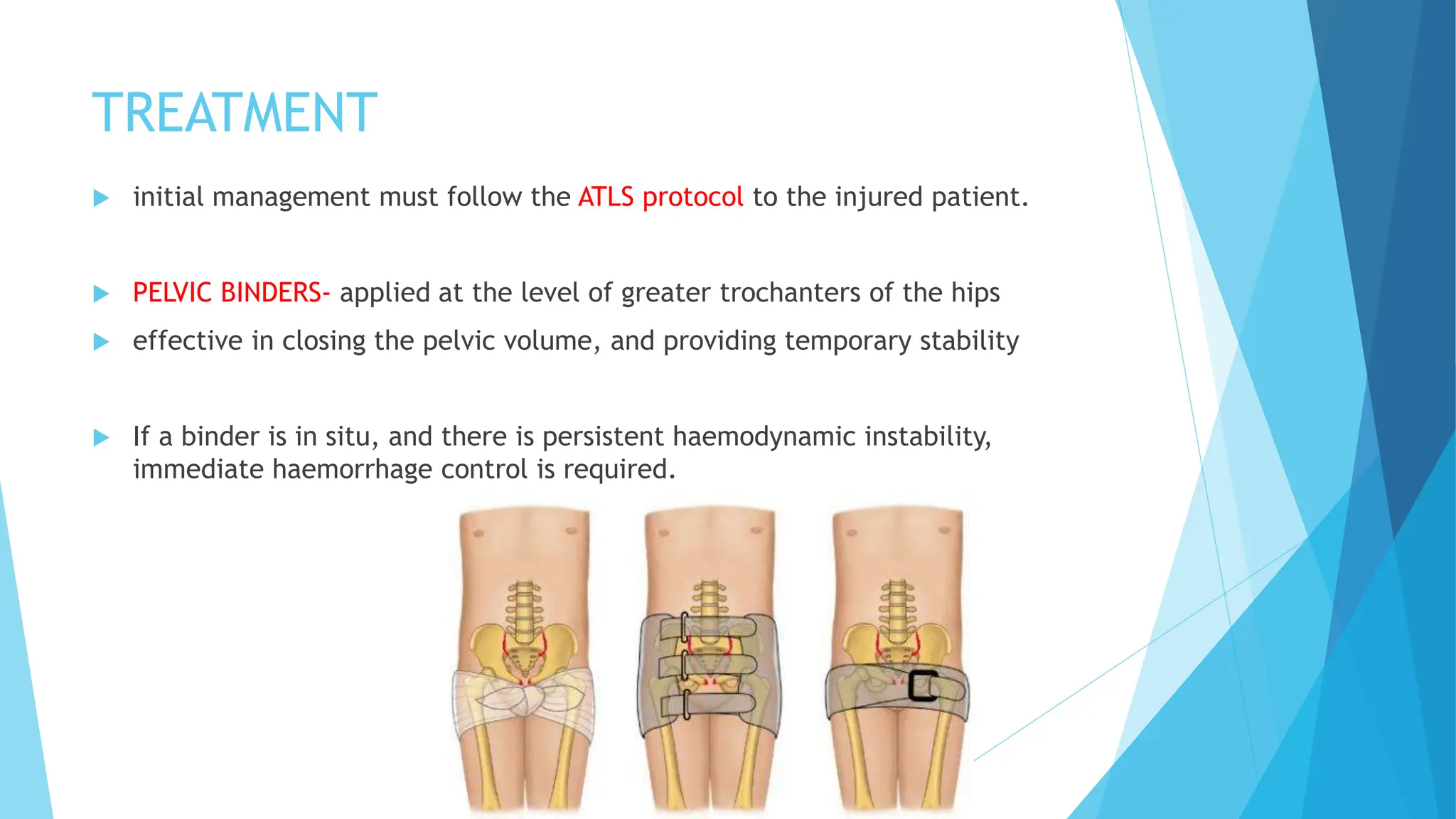
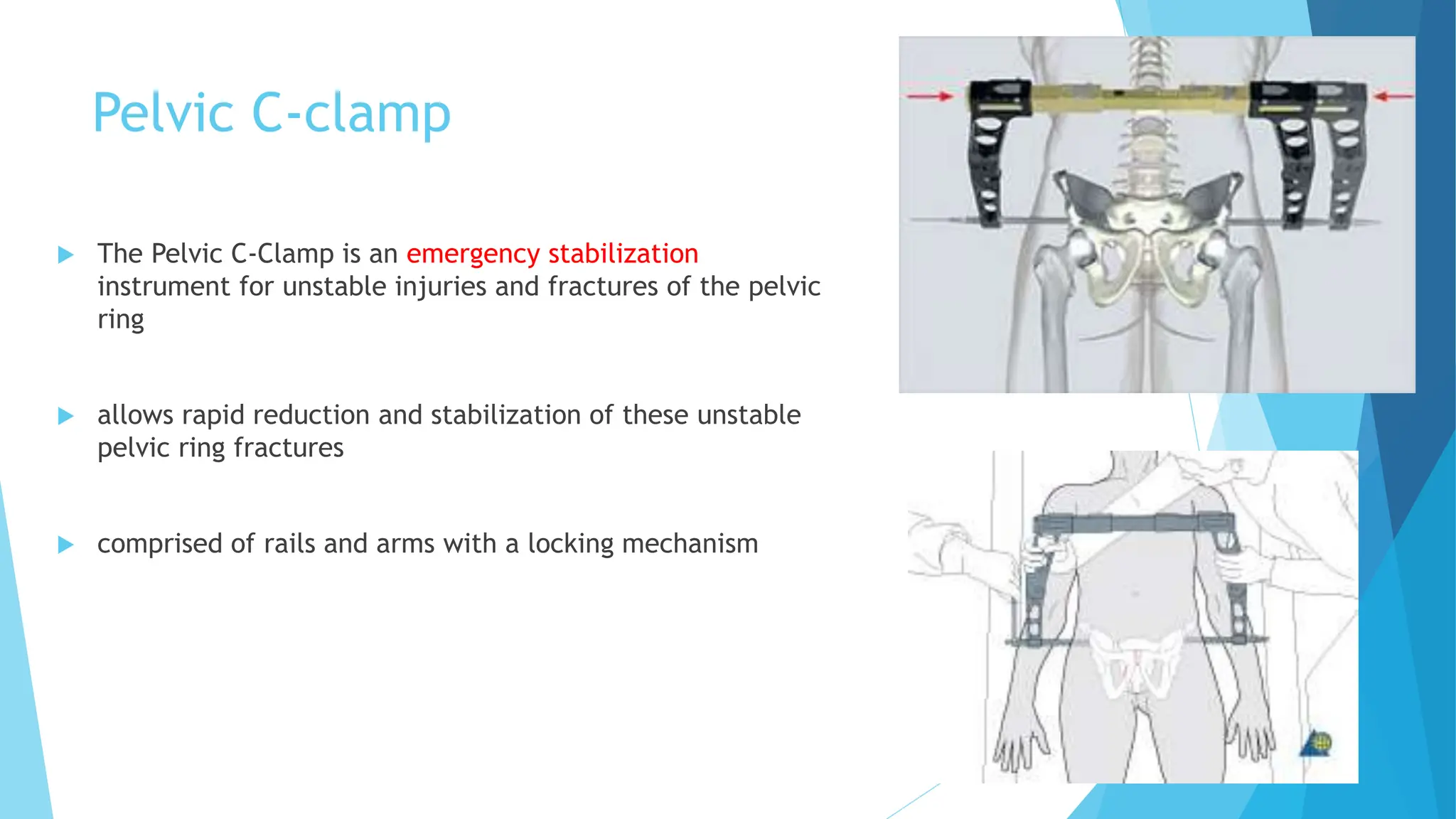
Pelvic fractures account for less than 5% of skeletal injuries but pose significant risks, including severe blood loss and associated visceral injuries. The management of pelvic fractures involves stabilization techniques such as pelvic binders and C-clamps, while imaging methods like X-rays and CT scans are vital for diagnosis and assessment. Acetabular fractures, often resulting from impact forces, are classified based on displacement and managed to restore joint congruency and stability to prevent long-term complications like osteoarthritis.