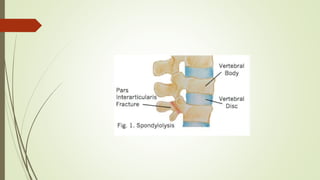
Spondylolysis is a stress fracture of the vertebra's pars interarticularis, which can lead to vertebral slippage and primarily affects young athletes, especially in sports requiring hyperextension. Symptoms include localized pain and restricted movement, typically relieved by rest, while diagnosis may involve imaging techniques like x-rays and SPECT scans. Management includes pain relief, cessation of aggravating activities, physical therapy, and in some cases, surgical intervention.