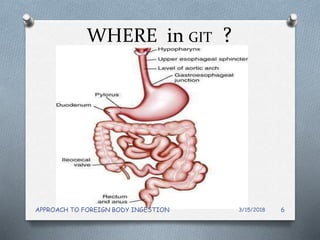
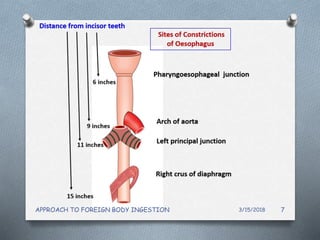
This document discusses the approach to foreign body ingestion. It begins with an introduction noting that foreign bodies in the gastrointestinal tract are generally not as dangerous as those in the airway. It then covers what types of objects are commonly ingested, who is most at risk, where in the GI tract objects typically lodge, clinical features, investigations like x-rays, and management approaches like endoscopic removal or conservative monitoring. Endoscopy is highlighted as the preferred minimally invasive method for removing ingested objects.