Downloaded 1,153 times

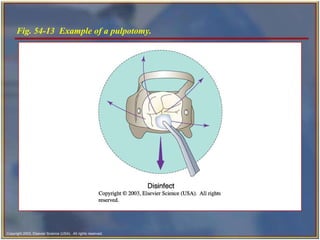
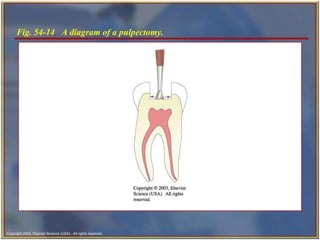


Endodontics is the specialty of dentistry that manages the dental pulp and surrounding tissues. It involves diagnosing and treating issues like pulpal nerve damage, which can cause pain or sensitivity. Diagnostic tests are used to examine the tooth and determine the specific condition, such as pulpitis or a periradicular abscess. Common endodontic procedures include pulpotomy, pulpectomy, and root canal therapy which aim to preserve or remove the pulp and disinfect and fill the root canals. Surgical endodontic procedures like apicoectomy and retrograde restoration are needed when non-surgical root canal treatment fails or to address anatomical issues.











































































































