![Treatment :
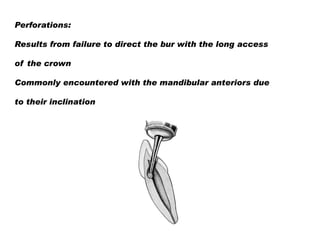
Lateral root perforations:
If above the crestal bone → good prognosis
Intracoronal placement of restorative material like
Glass ionomer, composite, MTA
Surgical exposure and sealing the defect externally
Below the crestal bone [coronal third of the root] →
Attachment loss →periodontal pocket
•
Crown lengthening/orthodontic extrusion to expose
the defect and repair](https://image.slidesharecdn.com/endomishaps12-140120060753-phpapp01/85/Endodontic-Mishaps-19-320.jpg)

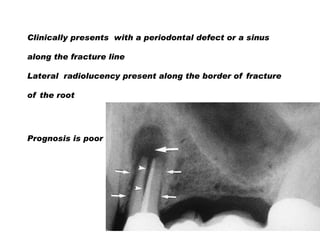
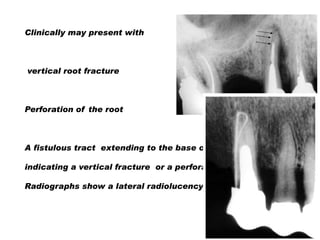
![Prognosis
Vertical root fractures ---------poor
Perforations----------good [surgically exposed and
sealed with MTA]](https://image.slidesharecdn.com/endomishaps12-140120060753-phpapp01/85/Endodontic-Mishaps-45-320.jpg)

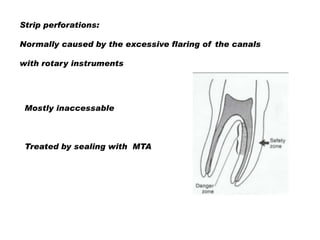
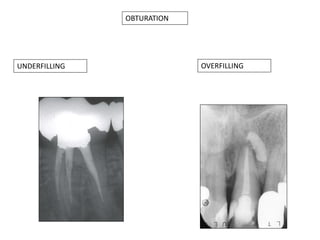
Endodontic mishaps include procedural errors that can occur during root canal treatment such as ledge formation, canal perforation, separated instruments, and overfilling/underfilling of canals. It is important for practitioners to understand how to recognize, prevent, and treat these mishaps. Common causes include inadequate access, excessive force, or improper instrument use. Perforations require immediate sealing with materials like MTA to achieve the best prognosis. Separated instruments may be bypassed or retrieved, while ledges can sometimes be circumvented with smaller files. Overall, minimizing errors requires adherence to principles like conservative access, copious irrigation, and careful instrumentation.






























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












