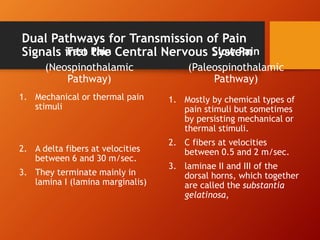
This document discusses pain perception and analgesia. It defines fast and slow pain, and describes the dual pathways for pain signal transmission - the fast A-delta fibers and slow C fibers. Pain is perceived when tissues are damaged and activates receptors. Pain is transmitted to the thalamus, cortex and reticular formation. The brain has an endogenous analgesia system using enkephalins to inhibit pain. Acupuncture and tactile stimuli can also induce analgesia. Referred pain causes perception of pain in remote areas. Visceral pain is often referred while parietal pain localizes to the source. Hyperalgesia enhances pain sensitivity. Various clinical pain conditions are also reviewed.