Downloaded 686 times
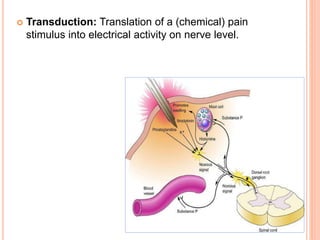
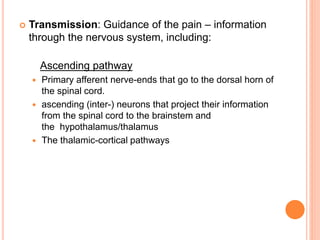
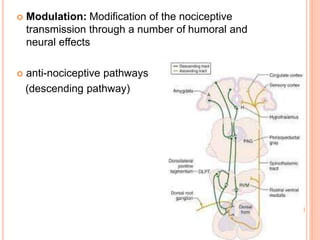
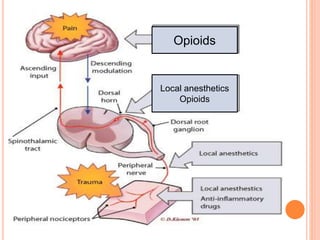
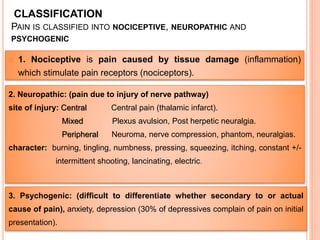
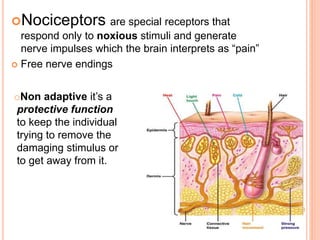

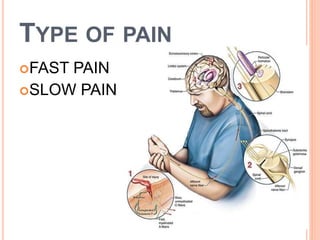

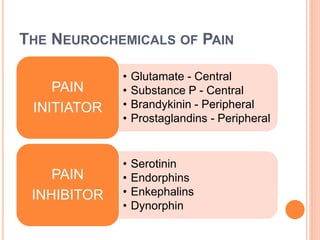
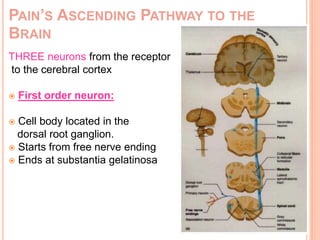
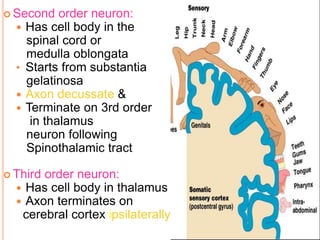
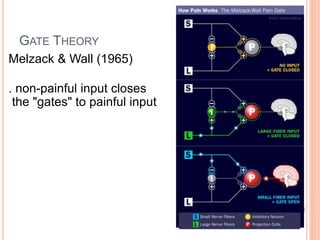
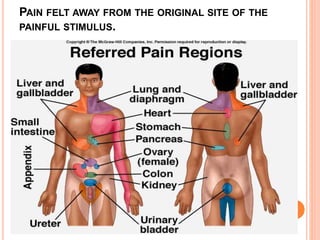

This document discusses pain anatomy and physiology. It defines pain as an unpleasant sensory and emotional experience associated with tissue damage. Nociception is the process by which nociceptors detect and transmit signals of potential tissue damage to the brain. There are different types of nociceptors and pain fibers that detect fast, sharp pain or slow, dull pain. The ascending pain pathway involves three neurons that transmit nociceptive signals from receptors to the spinal cord and thalamus. The gate control theory proposes that non-painful input can close the "gates" and inhibit pain transmission.






























































































