Download to read offline




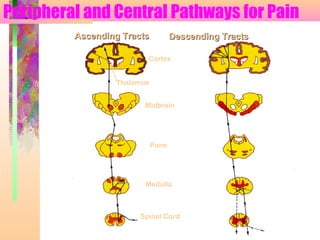

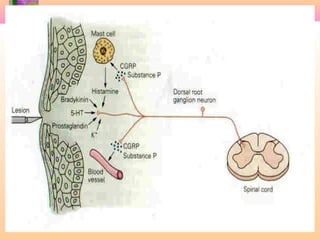

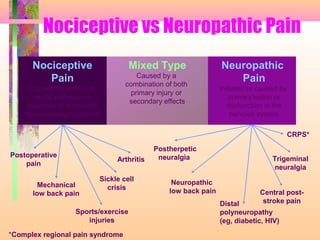











1. Pain is defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage. It is subjective and based on expectations, past experience, and emotional factors. 2. Pain is transmitted via nociceptors that detect extreme mechanical, thermal, or chemical stimuli and transmit signals along nerve fibers to the spinal cord and brain. 3. Chronic pain lasts longer than 6 months and is more complex, often involving altered anatomy and neural pathways. It is a lasting condition compared to acute pain which subsides with healing.













































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)
