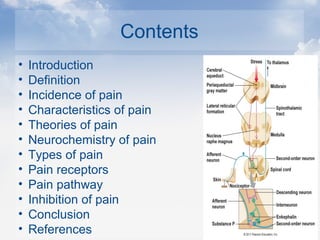
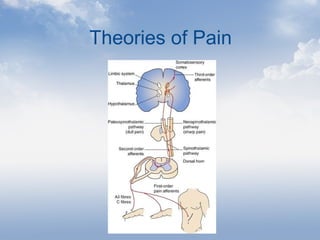
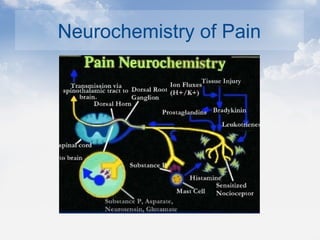
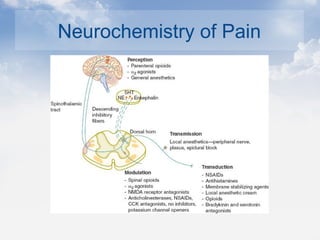
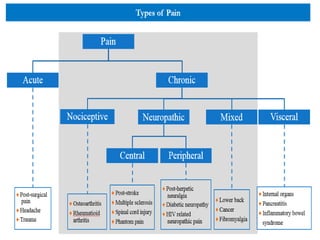
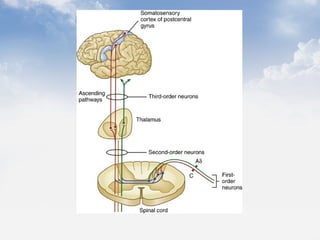
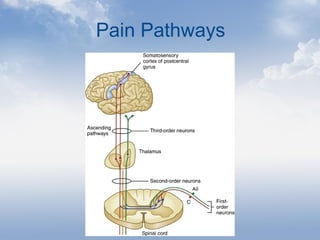
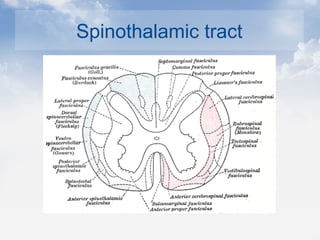
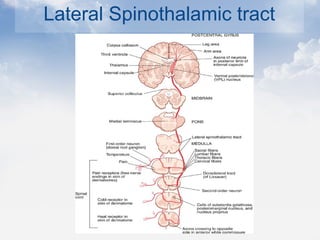
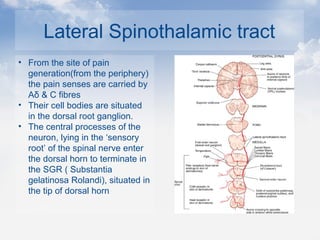
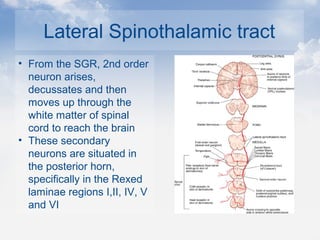
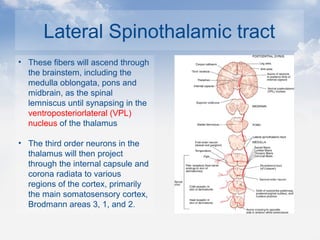
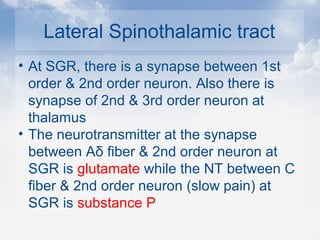
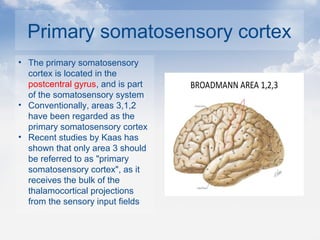
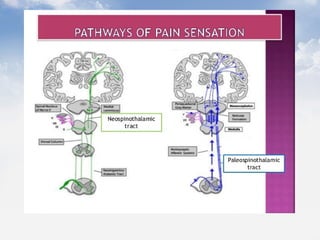
The document discusses pain and its pathways in the human body. It defines pain and describes its characteristics and theories. It discusses the neurochemistry and types of pain receptors. The main pain pathway described is the lateral spinothalamic tract, which carries pain and temperature sensations from the periphery to the thalamus and somatosensory cortex via the dorsal horn and spinal cord. It relays information via three orders of neurons and can be modulated in the substantia gelatinosa of the spinal cord.