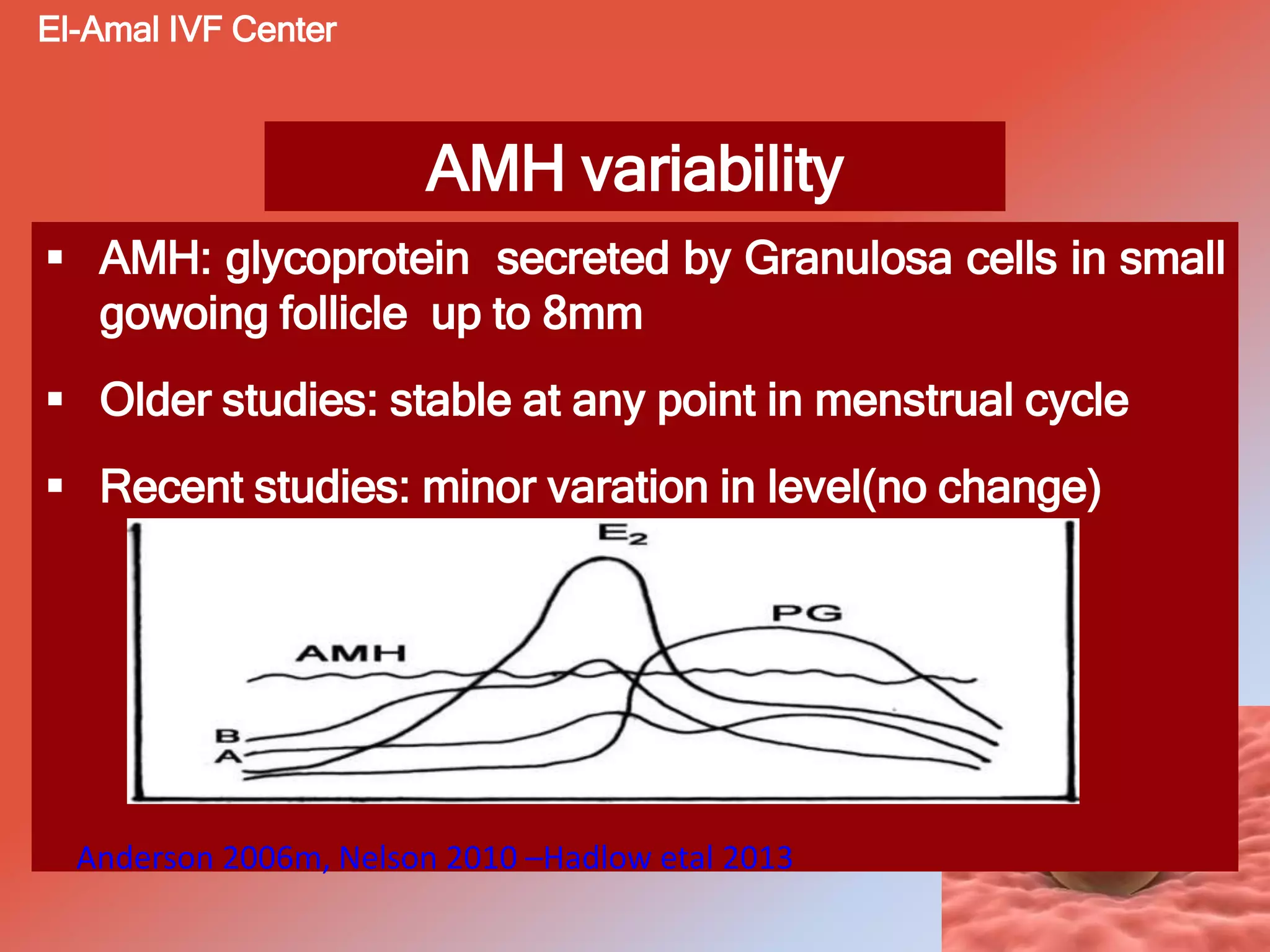
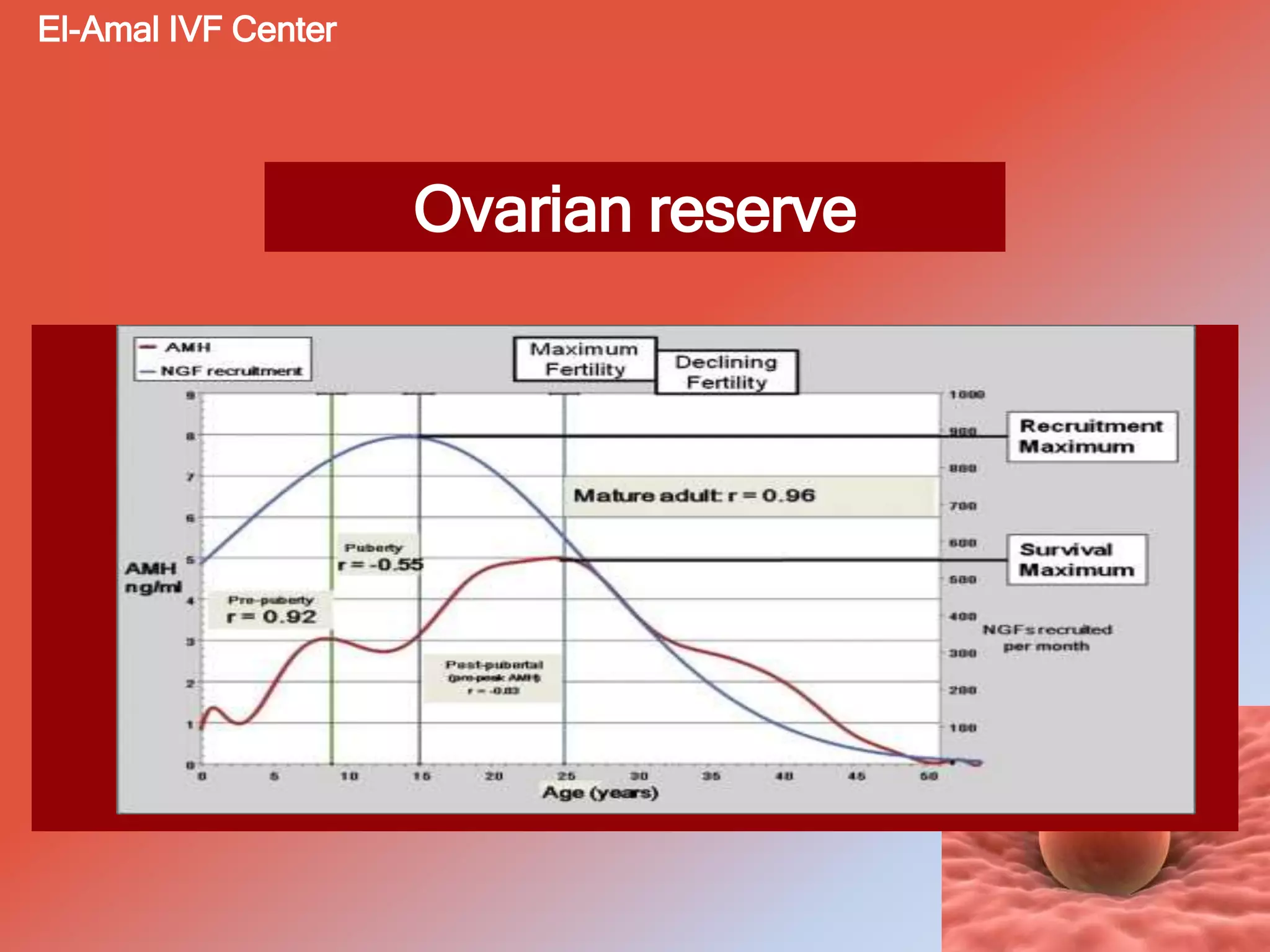
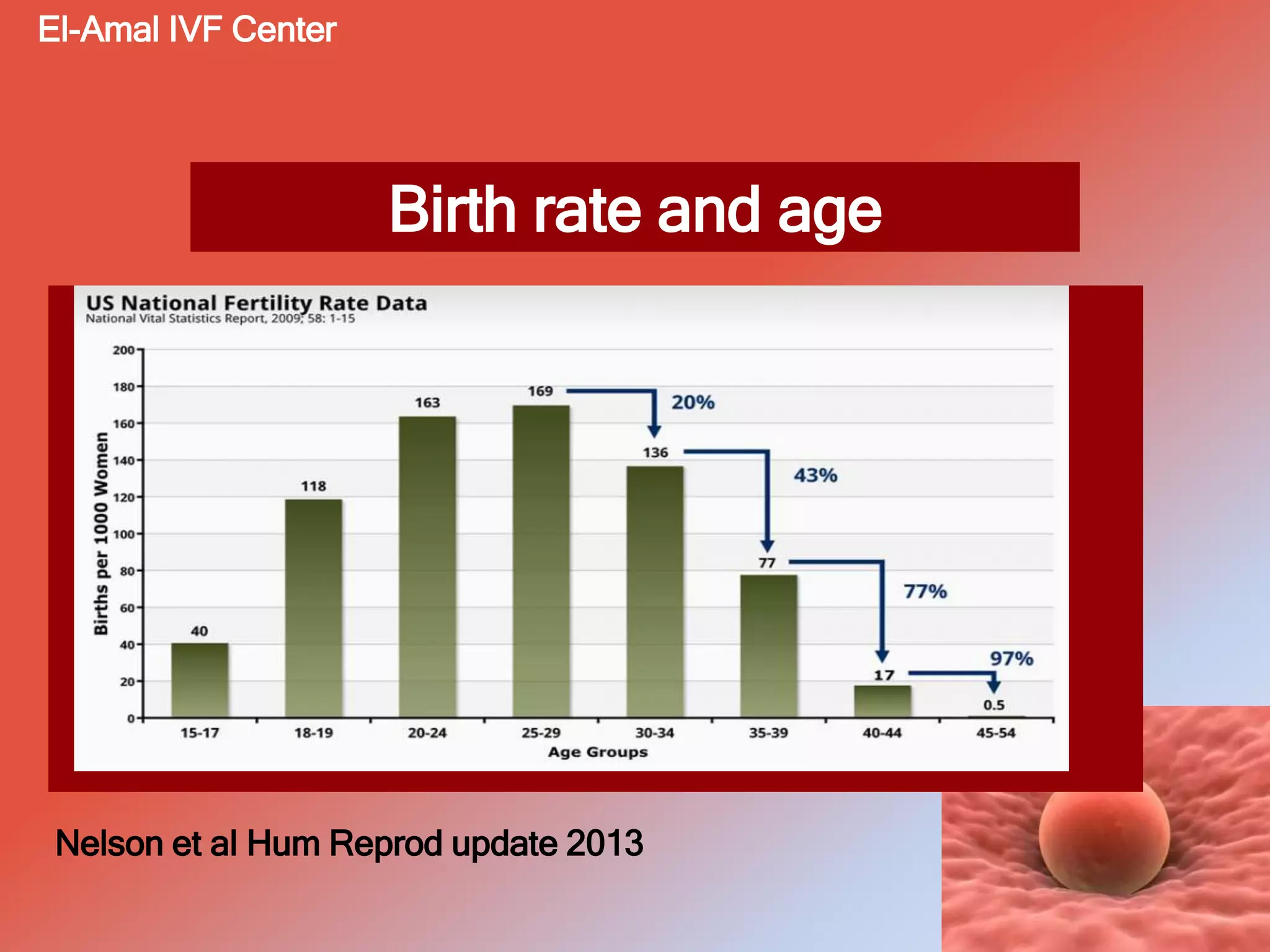
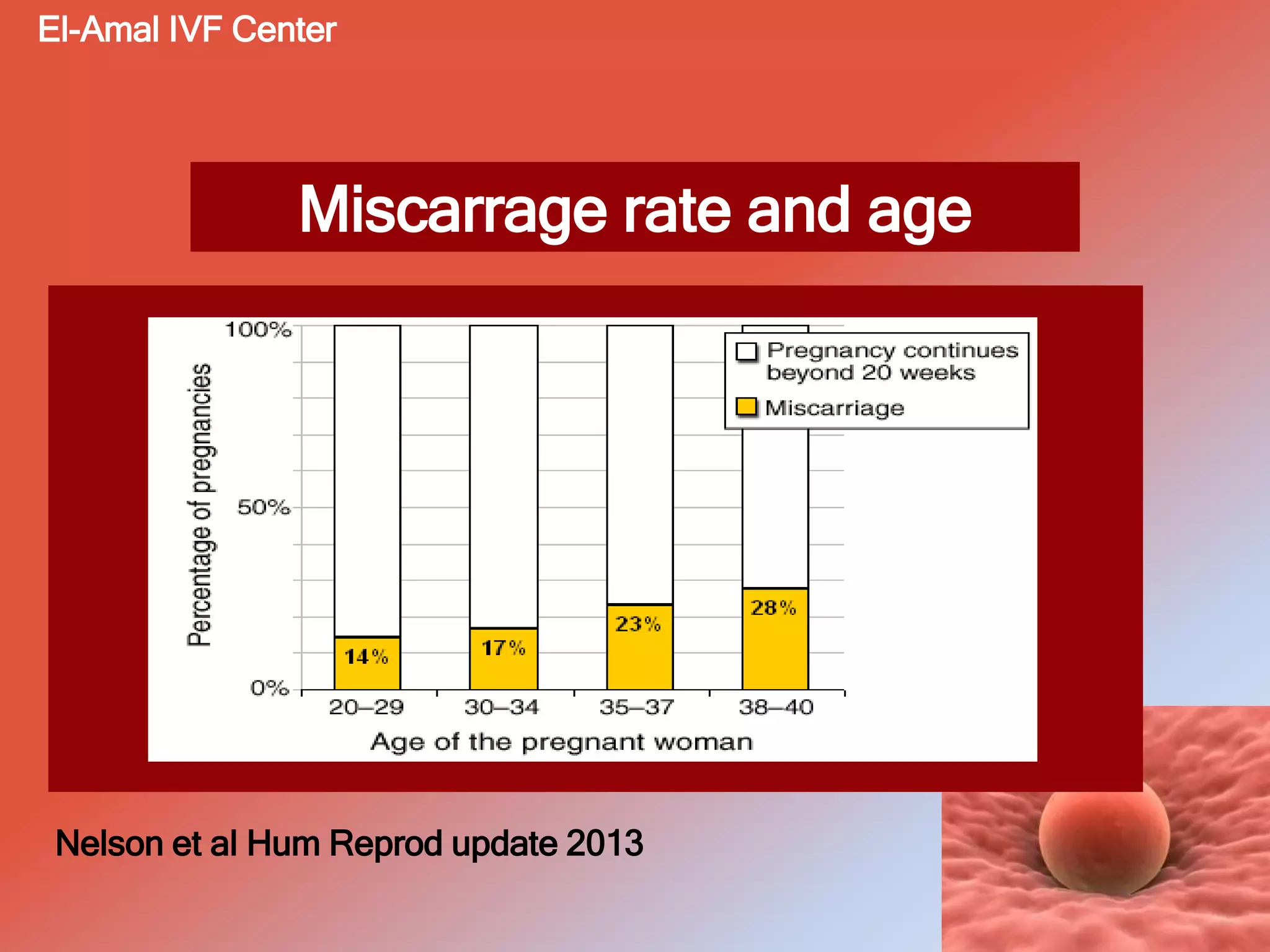
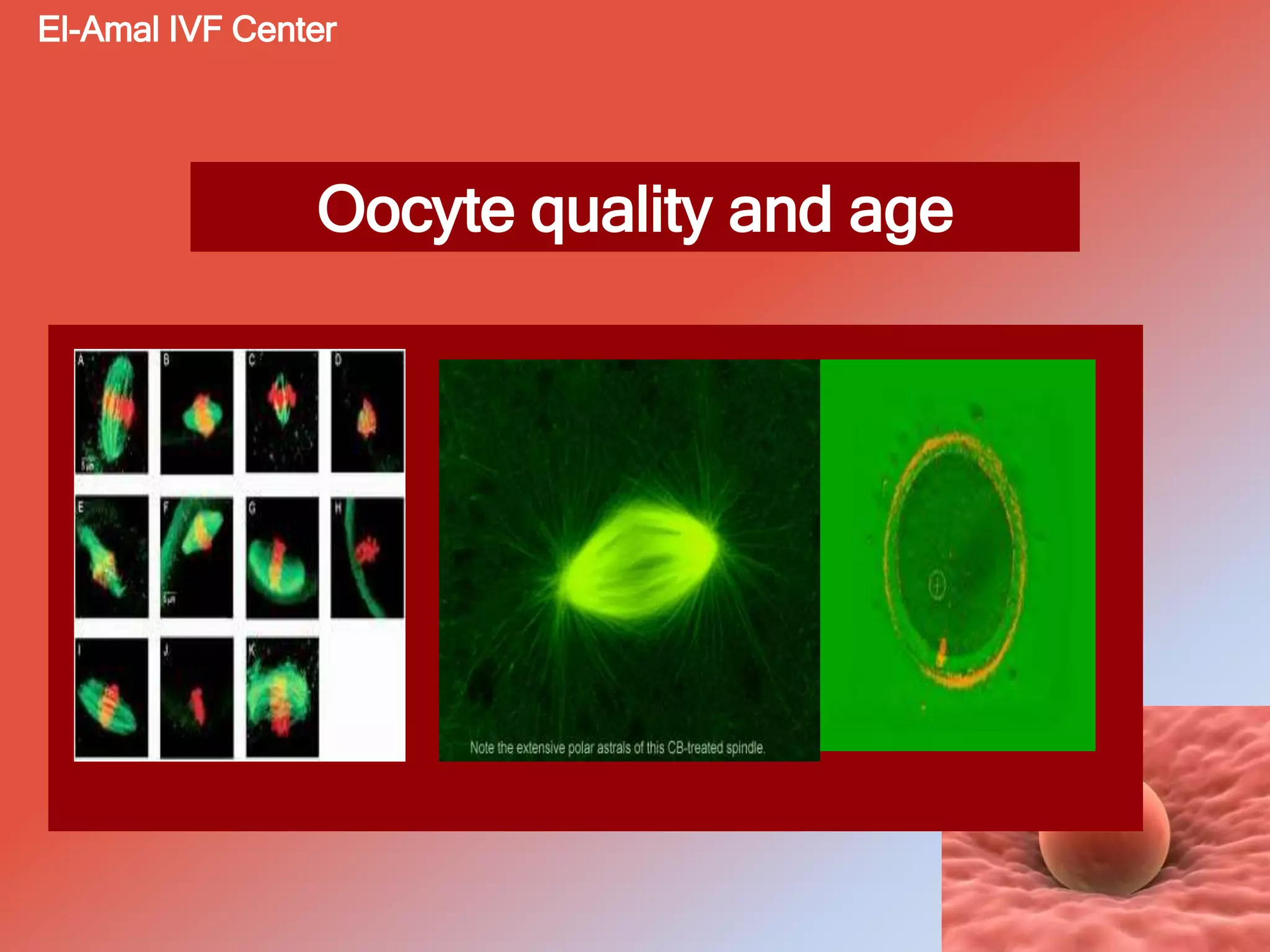
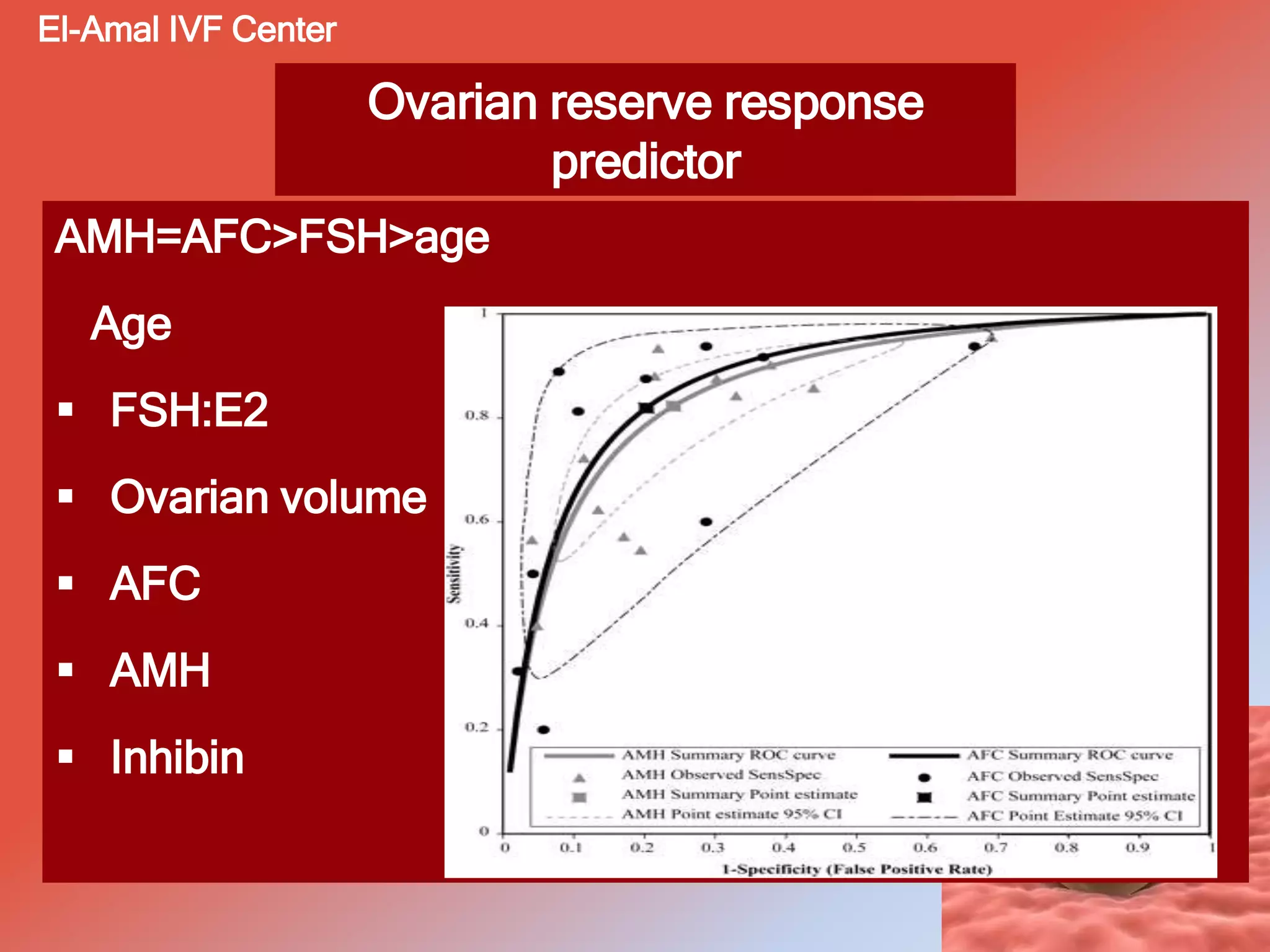
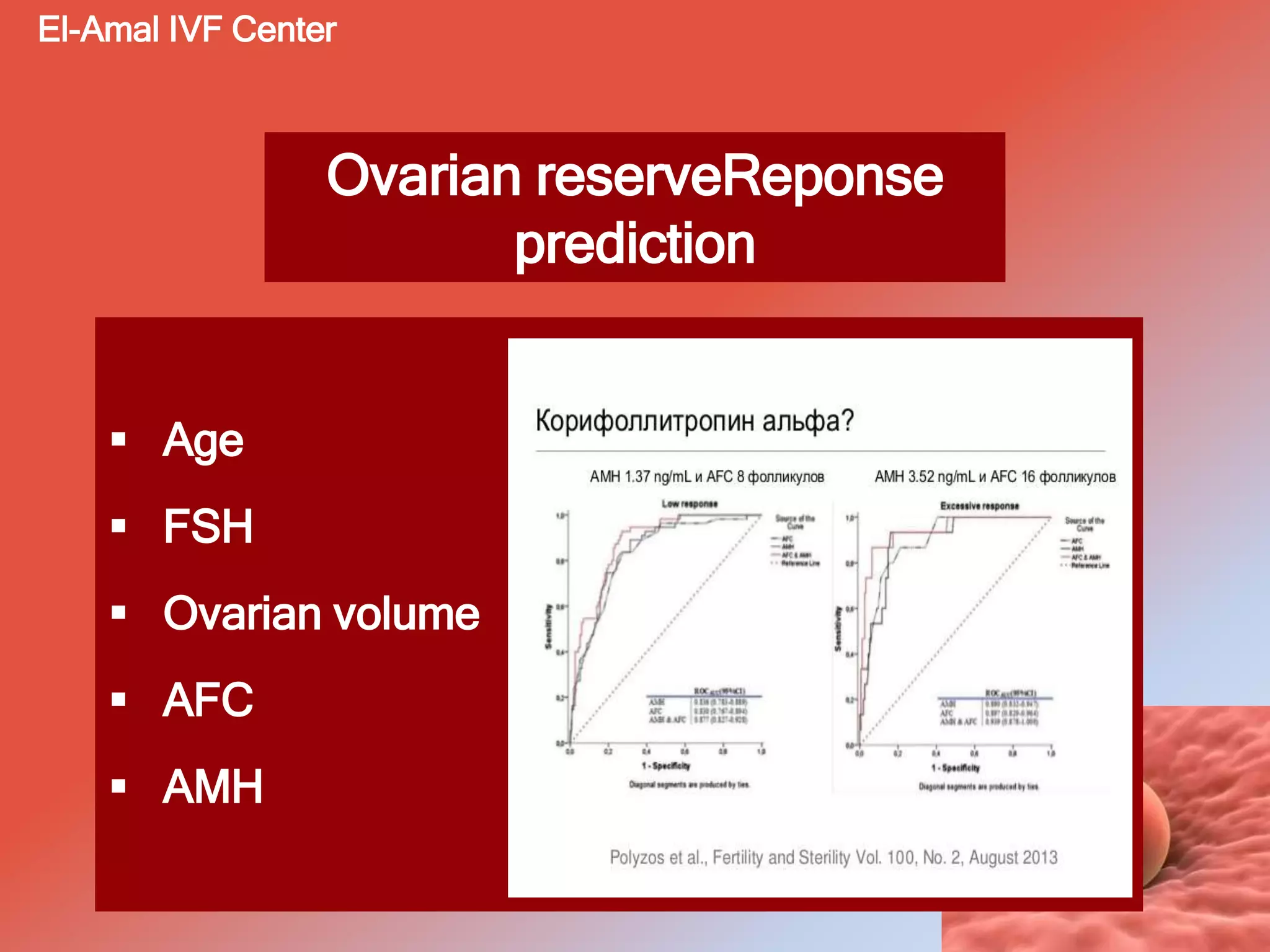
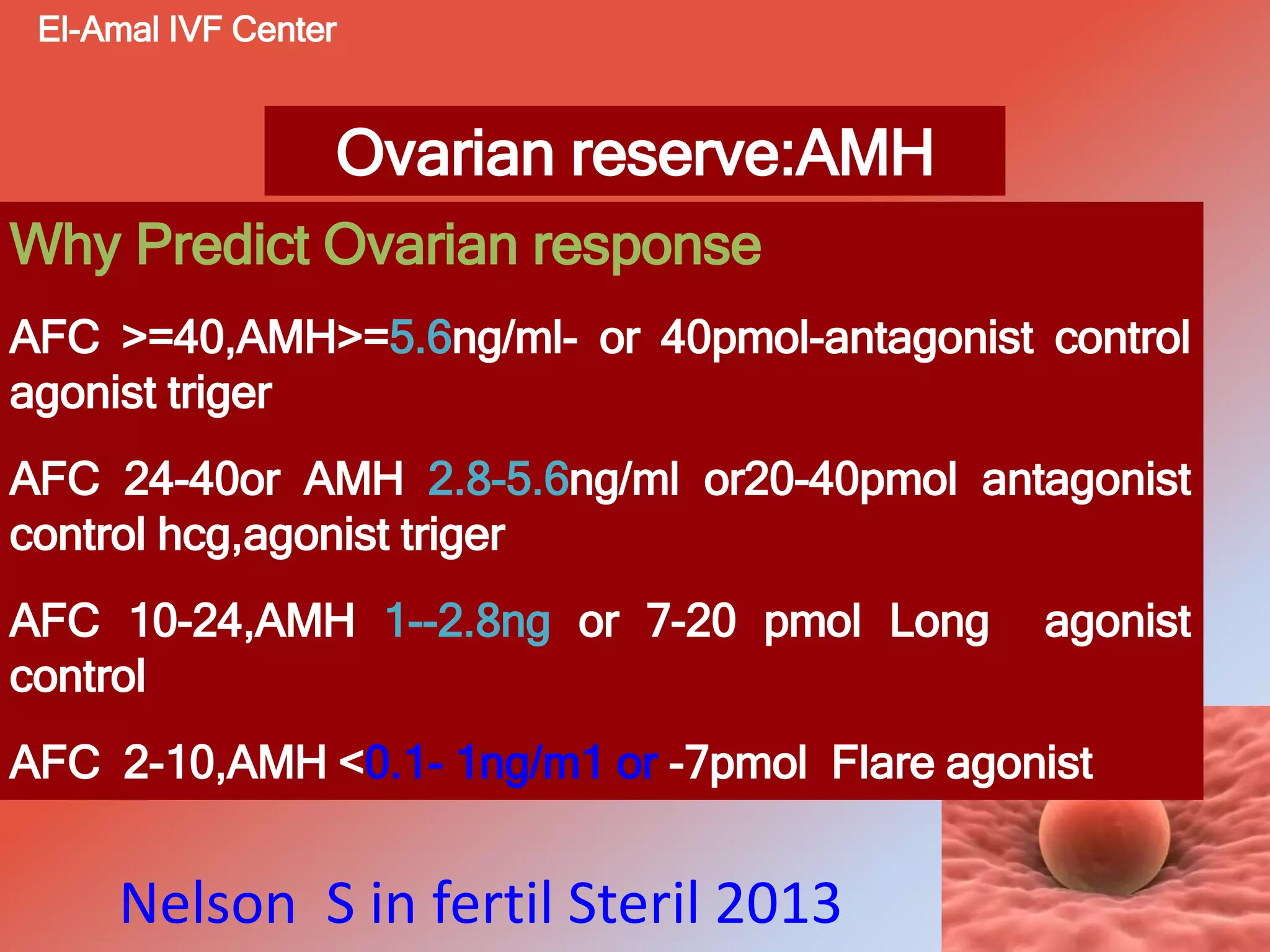
The document discusses the role of Anti-Müllerian Hormone (AMH) as a marker of ovarian reserve, highlighting its importance in predicting fertility outcomes and its variability in different health conditions. It covers topics such as the implications of AMH levels on fertility preservation, the effects of age and obesity on oocyte quality, and the utility of AMH in diagnosing conditions like polycystic ovary syndrome (PCOS) and granulosa cell tumors. Additionally, it outlines the limitations of AMH testing and suggests the need for individualized approaches in fertility treatments.