Downloaded 891 times














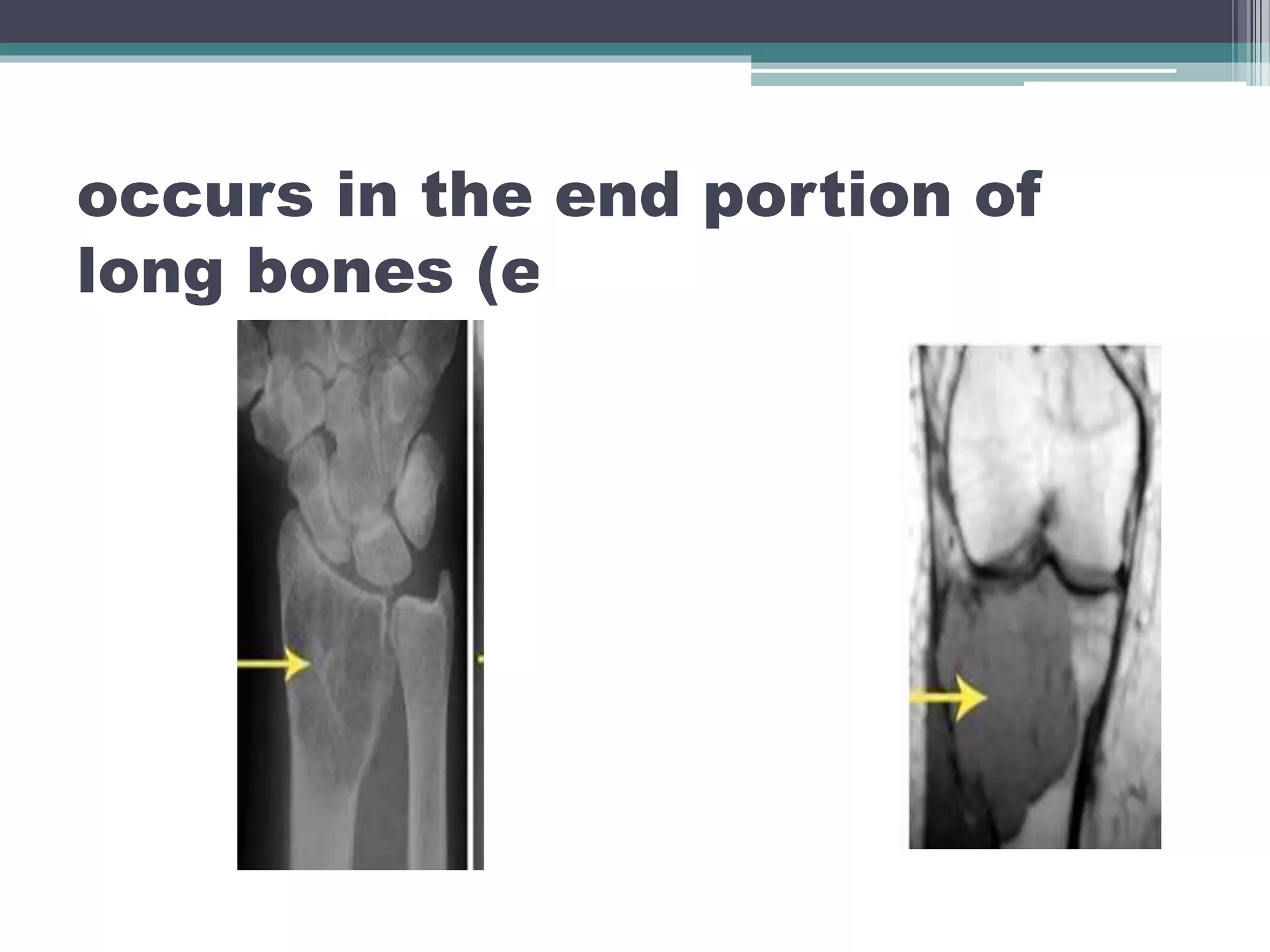




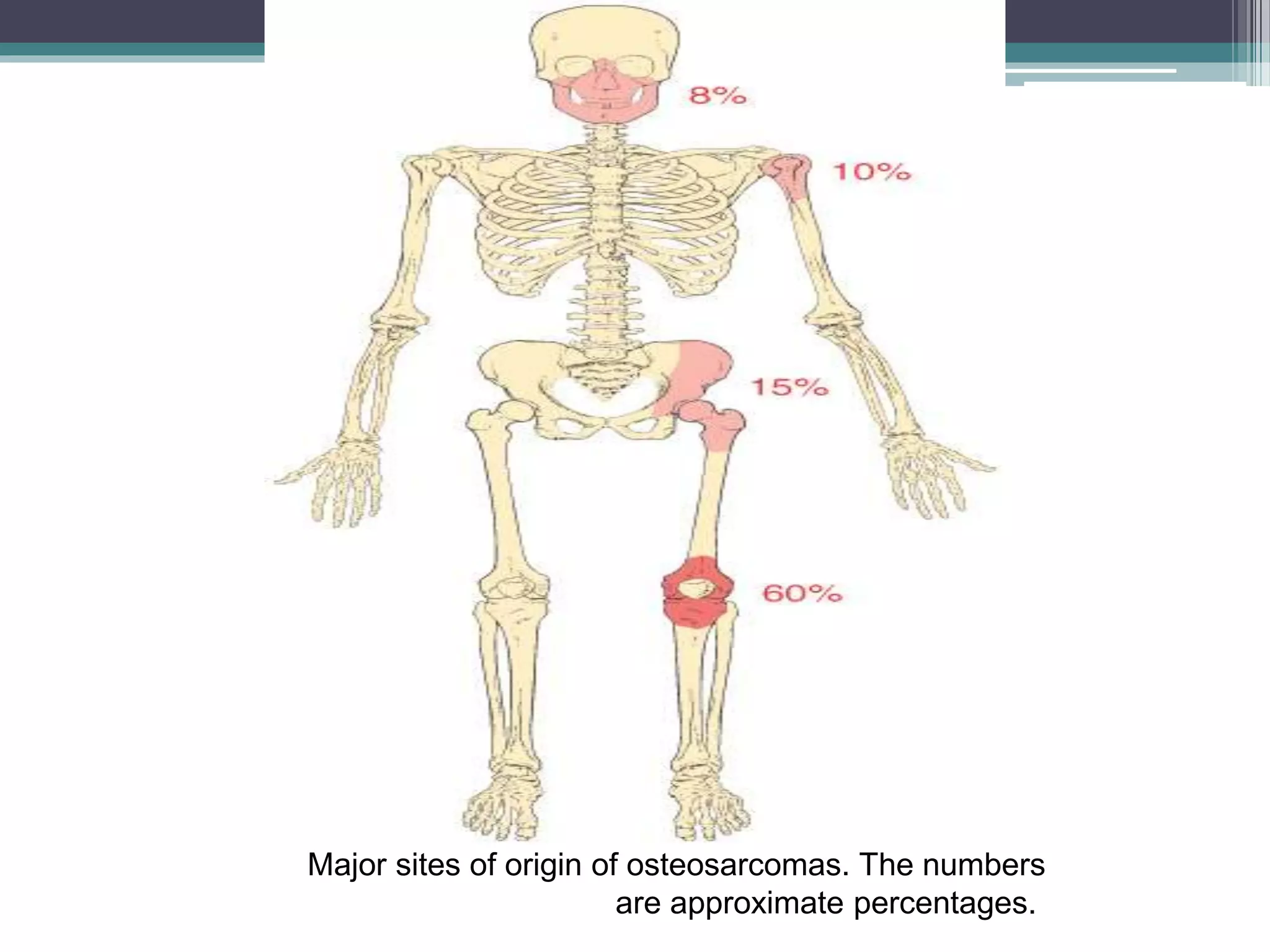

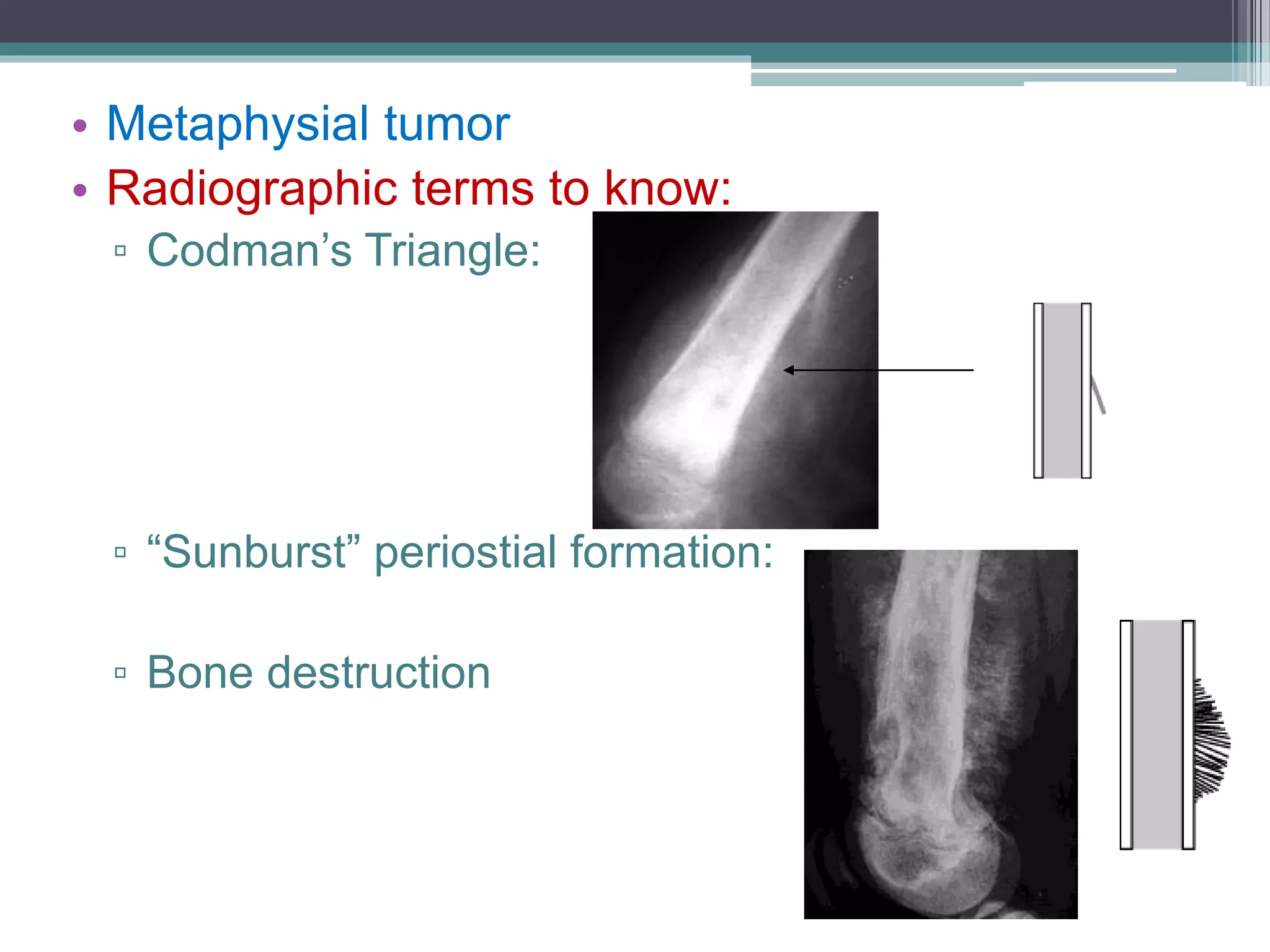
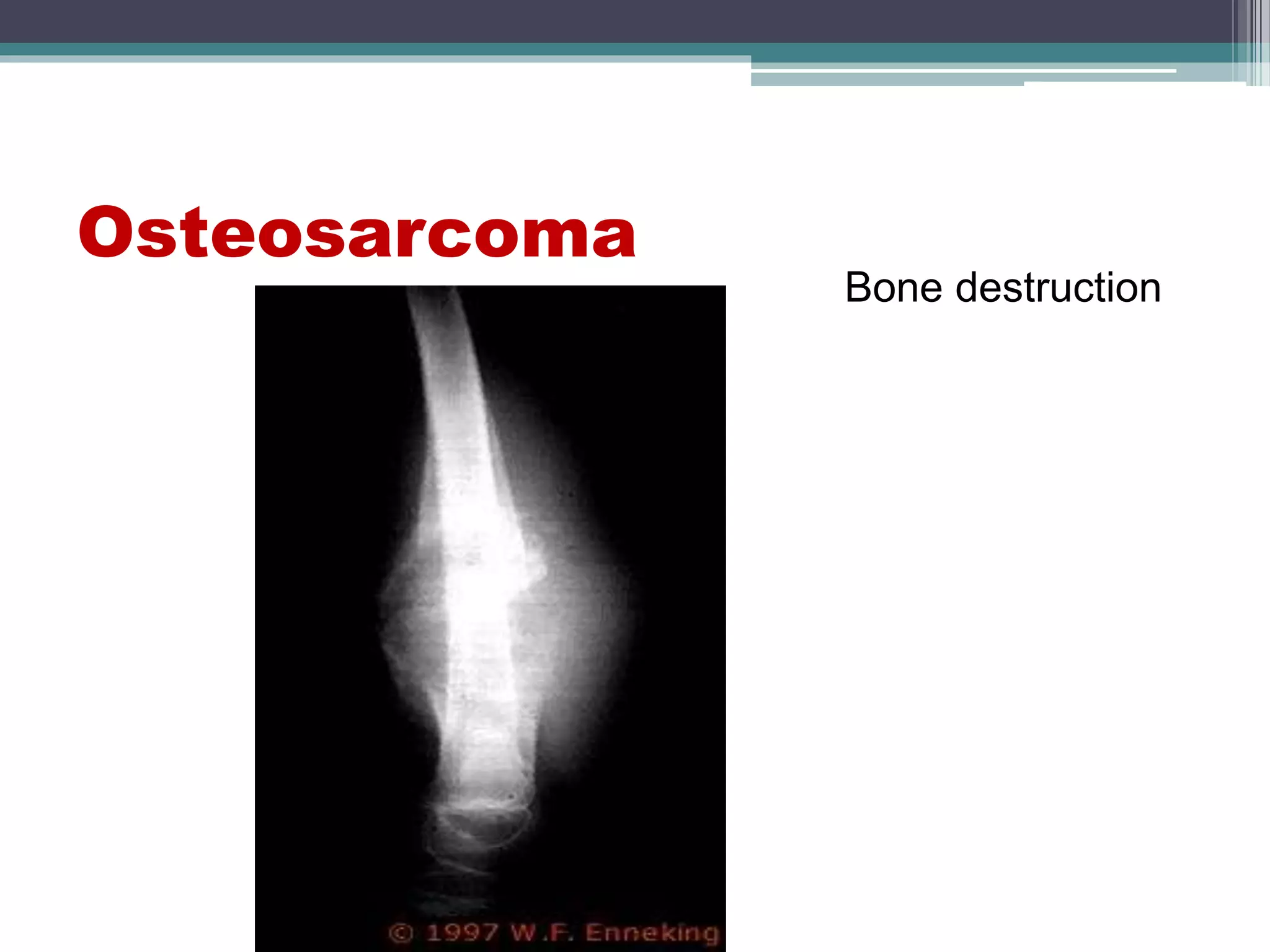













Bone tumors are abnormal growths in bone that can be benign or malignant, with most being benign and asymptomatic. Diagnosis typically involves radiographic analysis, and treatment varies based on the tumor type, with benign tumors often requiring no intervention unless symptomatic. Malignant bone tumors, such as osteosarcoma and multiple myeloma, present with more aggressive symptoms and necessitate more extensive treatment approaches.