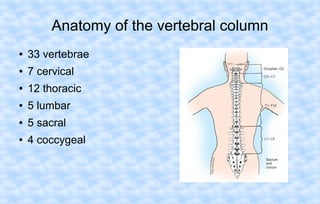
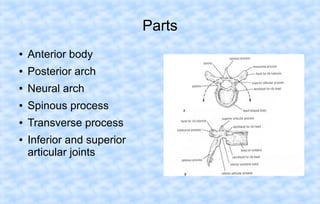
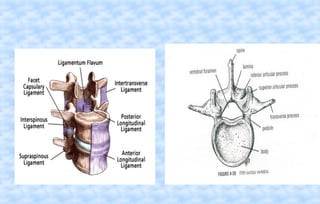
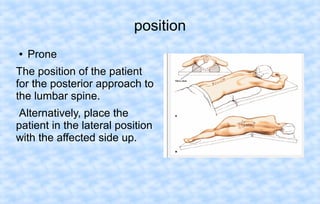
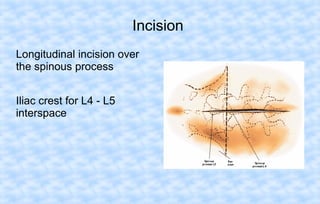
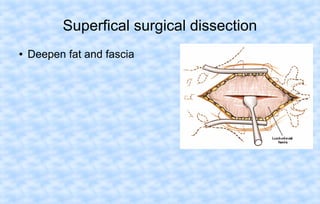
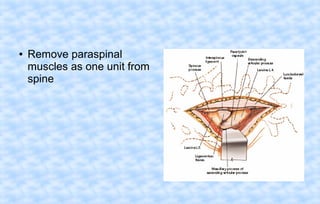
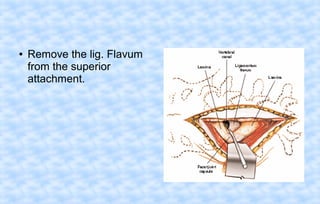
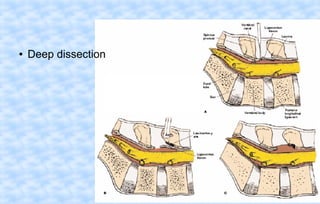
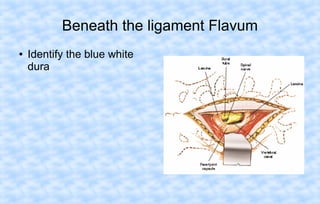
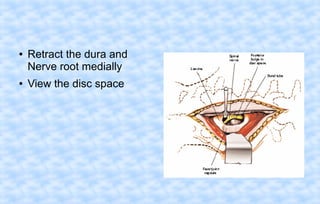
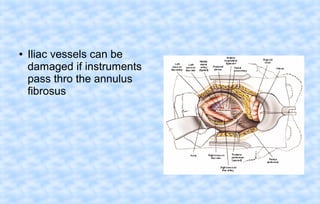
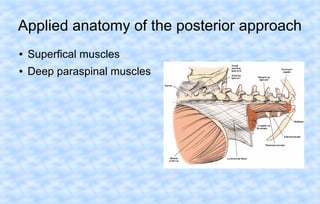
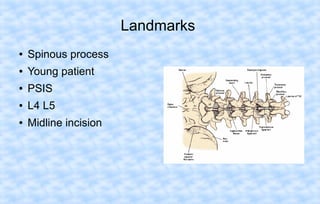
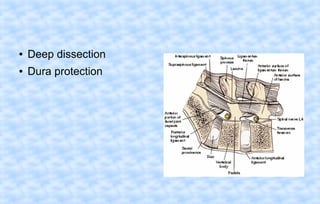
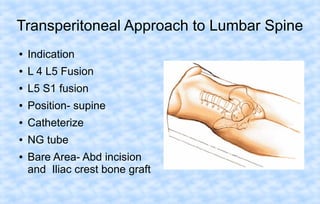
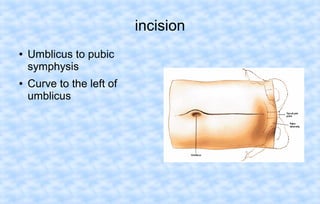
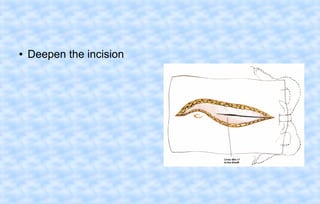
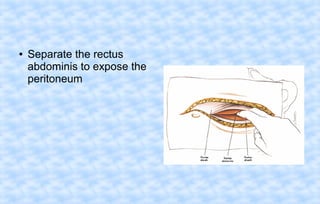
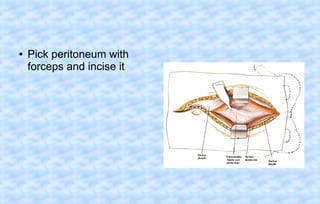
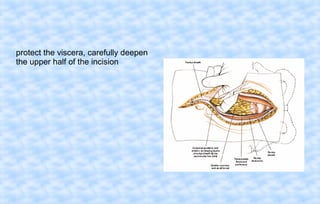
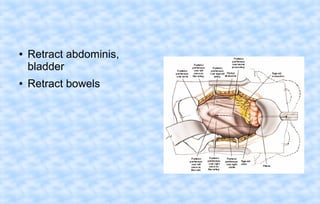
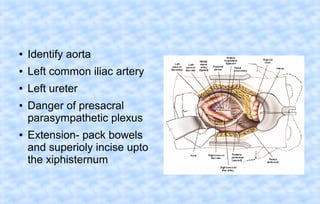
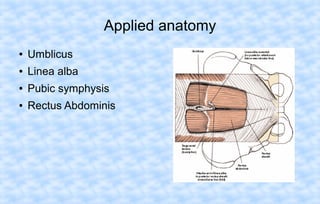
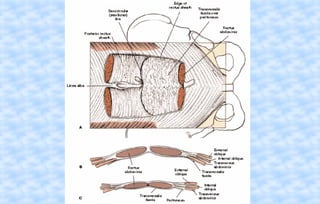
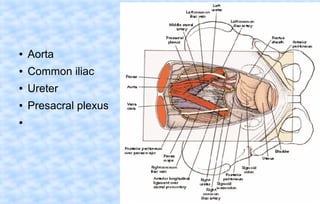
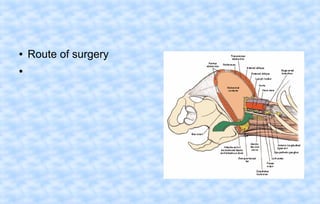
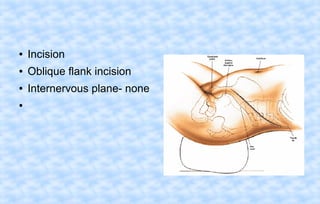
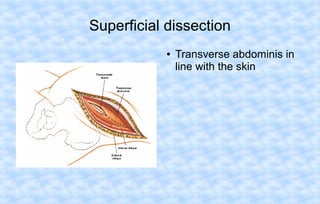
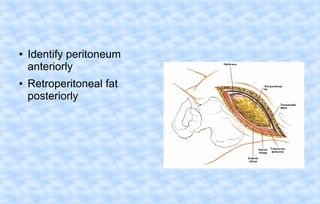
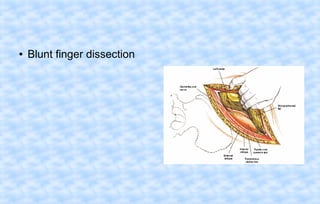
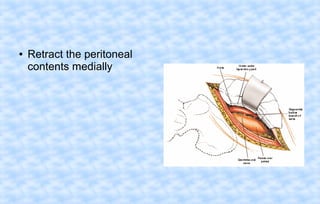
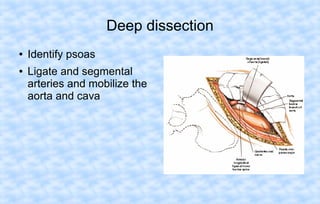
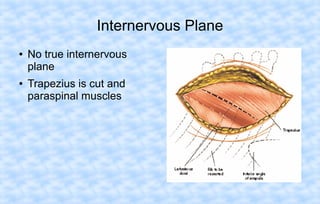
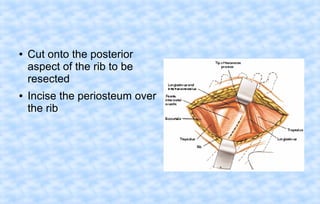
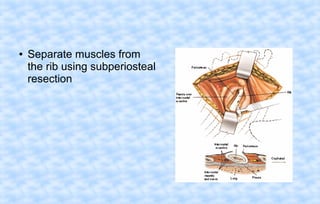
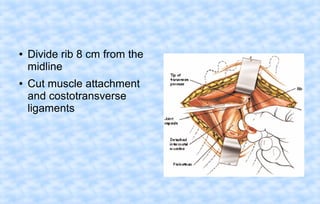
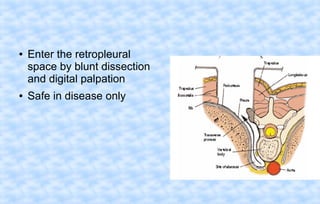
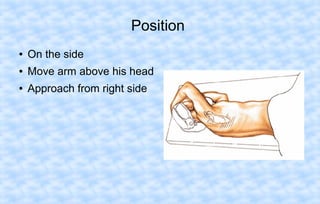
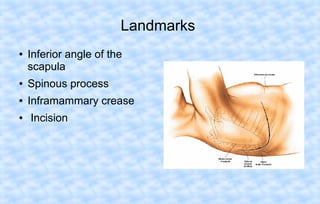
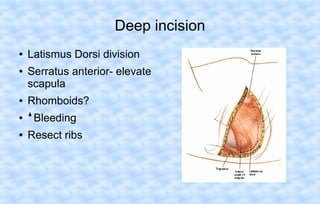
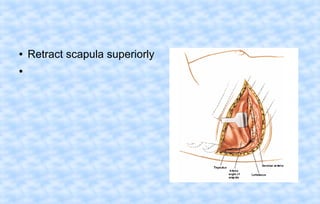
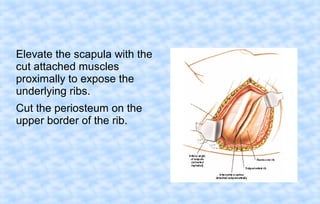
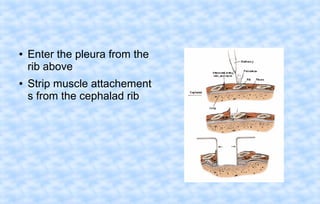
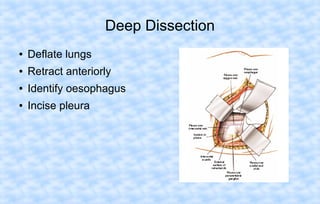
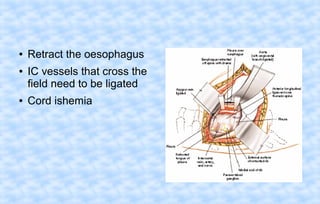
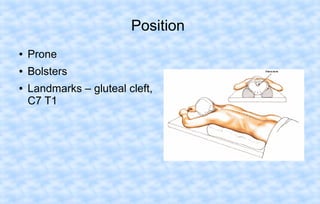
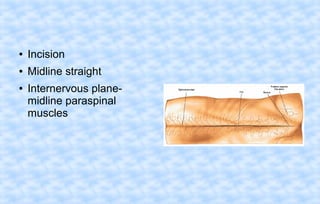
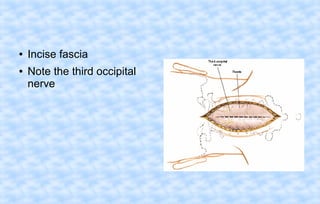
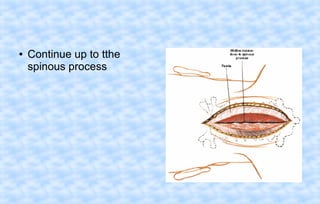
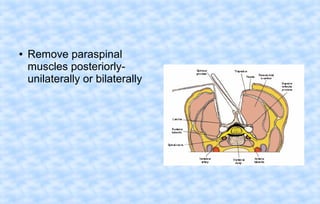
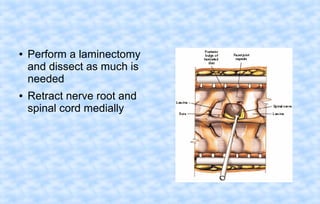
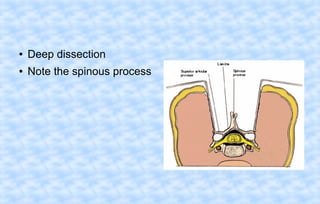
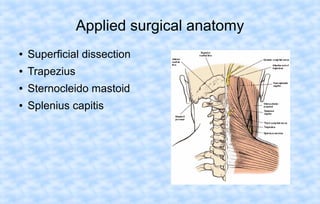
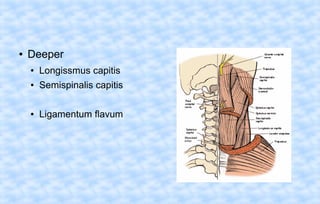
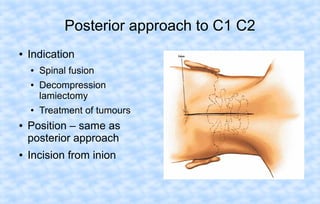
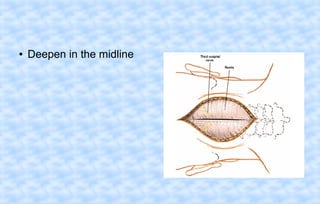
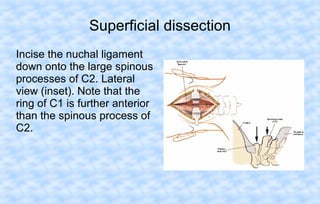
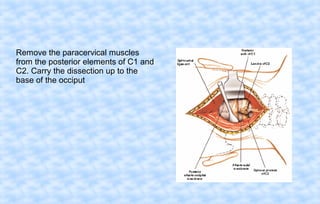
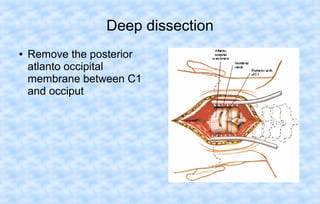
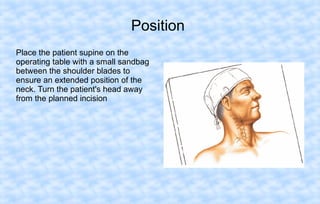
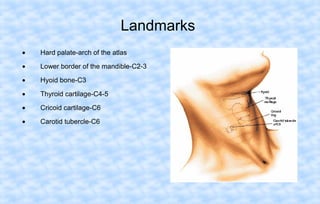
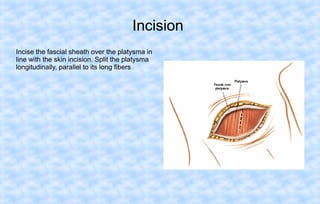
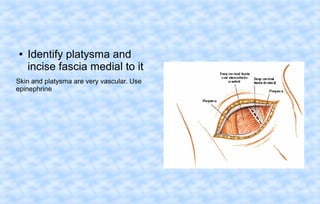
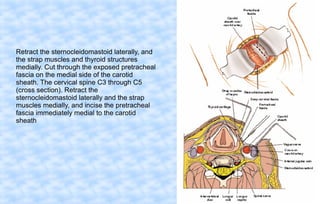
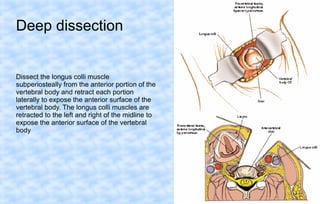
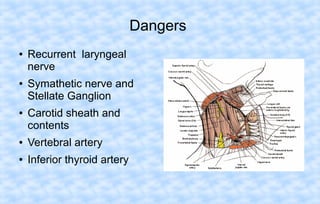
This document summarizes a seminar on approaches to the spine. It describes the anatomy of the vertebral column and parts of individual vertebrae. It then discusses several surgical approaches to different regions of the spine including the posterior, anterior, and lateral approaches to the lumbar spine, costotransversectomy and transthoracic approaches to the thoracic spine, and posterior approaches to the cervical and thoracic/lumbar spine for scoliosis correction. For each approach, it provides the indications, patient position, incision details, and dangers to watch out for. Applied surgical anatomy is also discussed.