Downloaded 44 times

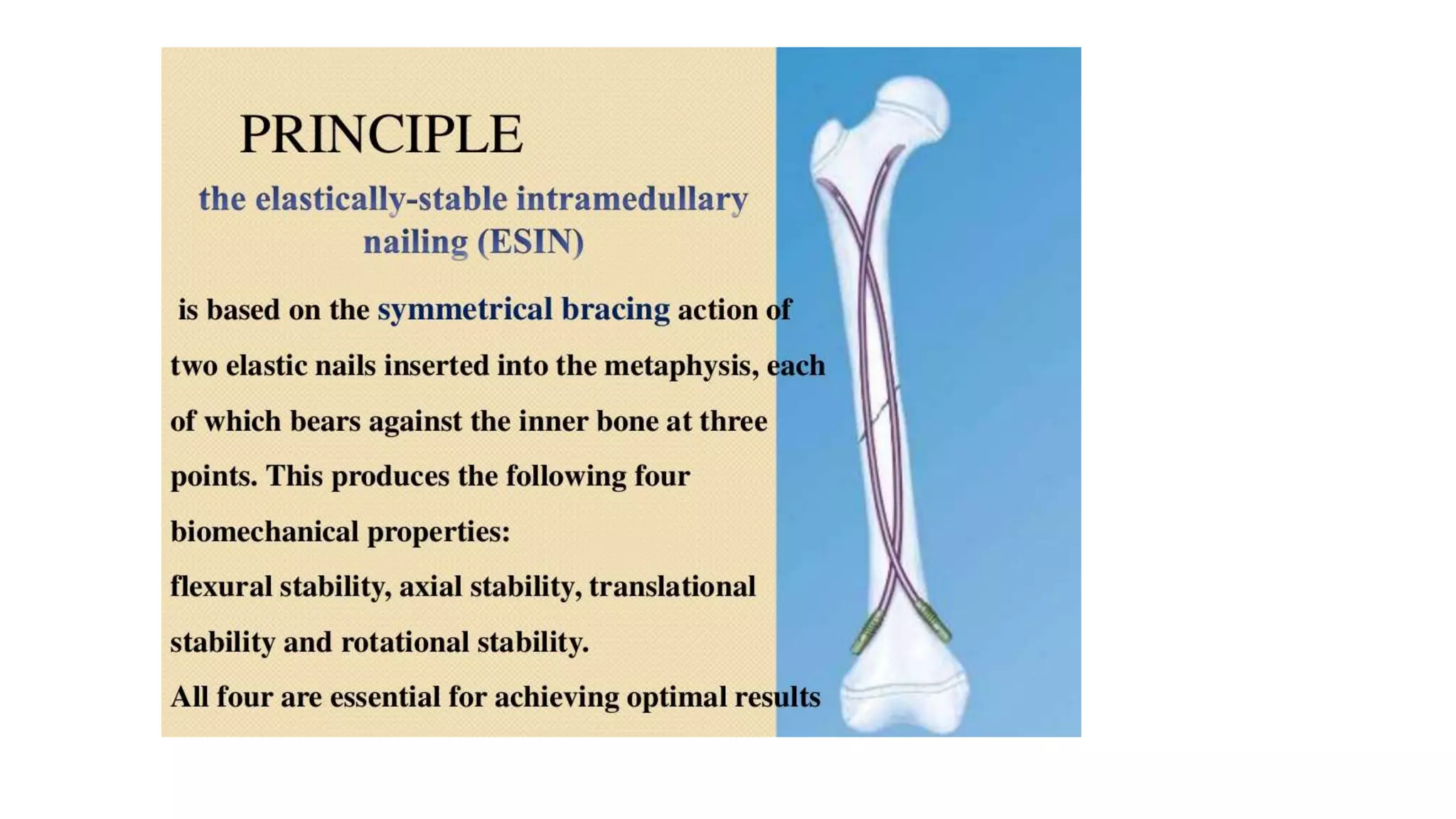

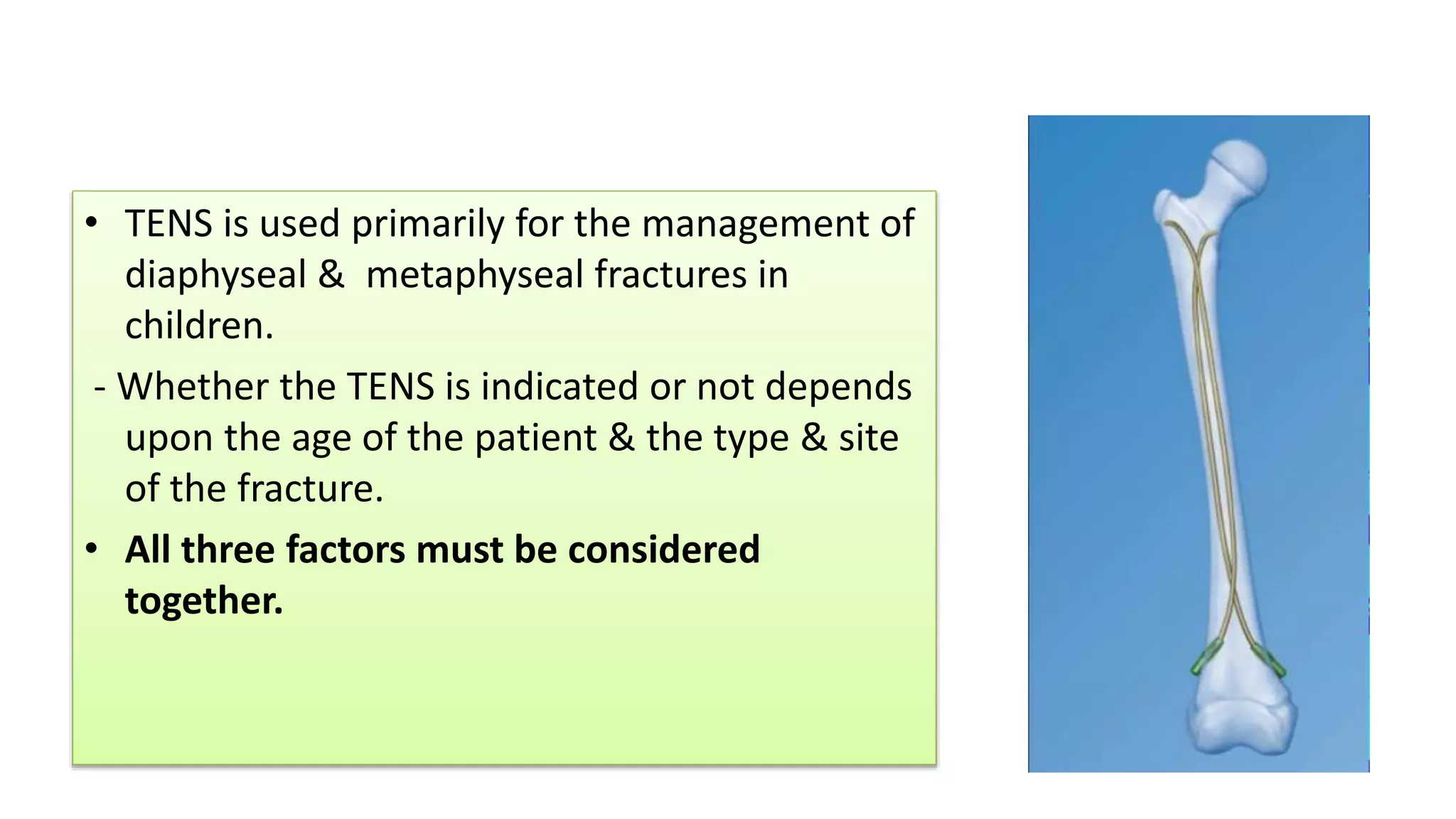












The document discusses the titanium elastic nailing system (TENS) used to treat fractures in children. TENS involves the use of flexible titanium nails inserted into the medullary canal. It is primarily used for diaphyseal and metaphyseal fractures in children ages 3-15. The appropriate use of TENS depends on considering the child's age as well as the type and location of the fracture. TENS provides stability while allowing bending and early ambulation.























































































