Downloaded 42 times

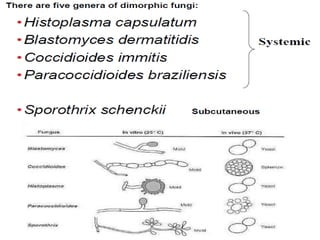
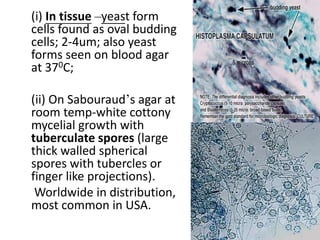
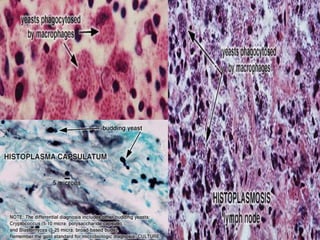
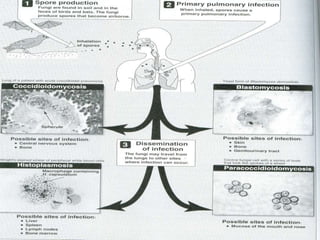

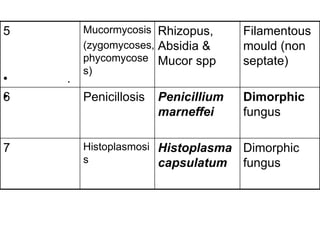

1. Systemic fungal infections originate at one site like the lungs and disseminate to other body sites. They are caused by soil fungi that are dimorphic, existing in both mold and yeast forms. 2. Histoplasmosis is caused by the dimorphic fungus Histoplasma capsulatum. It is acquired through inhalation and causes pulmonary and disseminated infection, especially in those with impaired immunity. 3. Opportunistic mycoses mainly affect immuno-compromised individuals and are becoming more common due to immunosuppressive treatments, HIV/AIDS, and antibiotic overuse. Common opportunistic fungi include Candida, Cryptococcus, Aspergillus, and M























































































