Downloaded 42 times



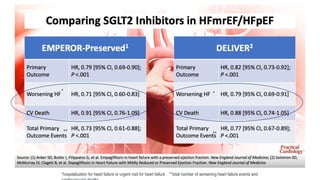
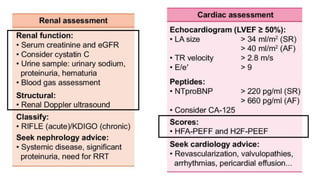
![Cardiorenal Interactions : A Historical Note
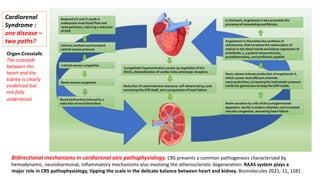
In 1842, Carl Ludwig proposed the hypothesis that urine is
the result of a filtration process by the glomeruli promoted
by the force of blood pressure
[Ludwig, C. De Viribus Physicis Secretionem Urinae Adjuvantibus: Commentatio Quam Pro
Venia Legendi Gratioso Medicorum Marburgensium Ordini. Elwert. 1842. ]
Carl Ludwig
(1816–1895) ,
a pioneer of physiology ,
presented a new
concept of renal
function and cardiorenal
interaction.](https://image.slidesharecdn.com/hfpefckd-mima2022-221022074558-bea51cca/85/Linking-HFpEF-and-Chronic-kidney-disease-5-320.jpg)


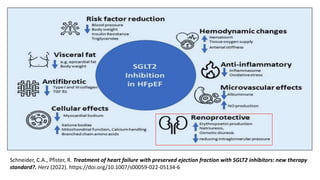
![55
50
45
40
35
30
25
20
15
10
5
0
Mean
Cumulative
Events
per
100
patients
0
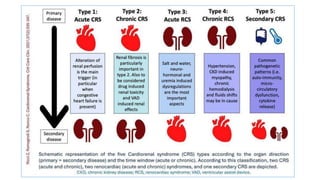
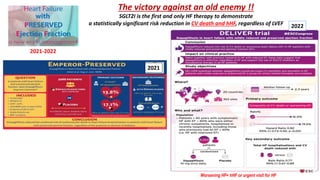
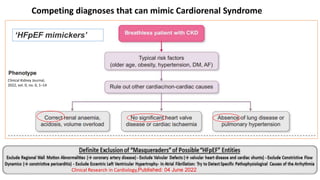
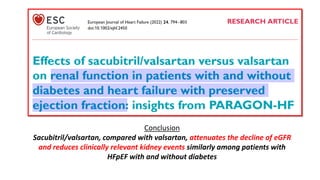
*Semiparametric LWYY method. CV,
cardiovascular; HF, heart failure
Solomon S, et al. N Engl J Med. 2019 (In press)
1 2
Years
3 4
Valsartan (n = 2389)
1009 events, 14.6 per 100 pt-years
Sacubitril/valsartan (n = 2407) 894 events,
12.8 per 100 pt-years
13% reduction in the risk of the primary endpoint
(rate ratio [RR]: 0.87; 95% CI: 0.75 to 1.005; p=0.058)
Primary endpoint: Recurrent event analysis of total HF hospitalizations and CV death*
Sacubitril–valsartan did not result in a significantly
lower rate of total hospitalizations for heart failure and
death from cardiovascular causes among patients with
heart failure and an ejection fraction of 45% or higher.](https://image.slidesharecdn.com/hfpefckd-mima2022-221022074558-bea51cca/85/Linking-HFpEF-and-Chronic-kidney-disease-49-320.jpg)


![Russian novelist & poet
[born 1818, died 1883]
The coexistence of CKD in HFpEF (CRS type 2 and 4) : Cardio-Renal Clinical Challenges](https://image.slidesharecdn.com/hfpefckd-mima2022-221022074558-bea51cca/85/Linking-HFpEF-and-Chronic-kidney-disease-75-320.jpg)

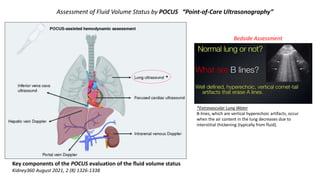
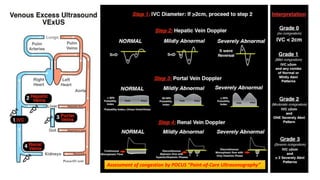
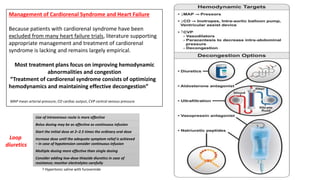
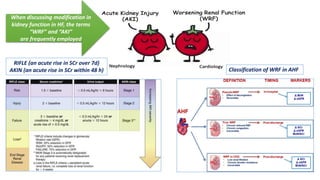
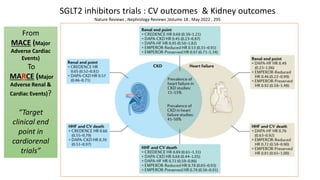
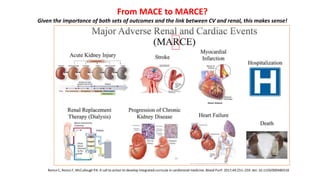
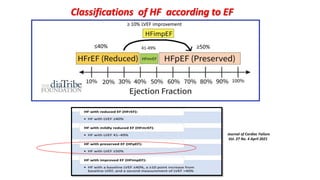
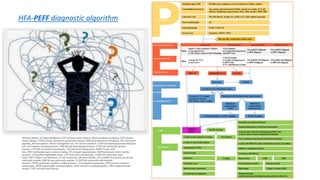
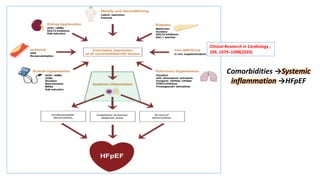
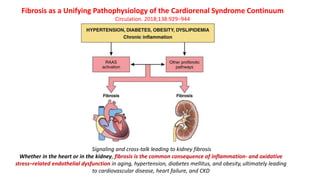
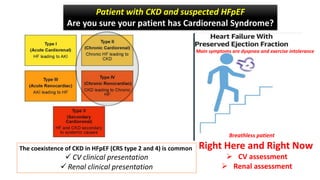
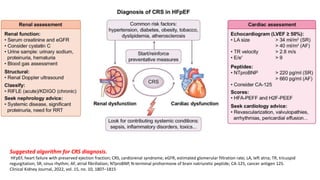
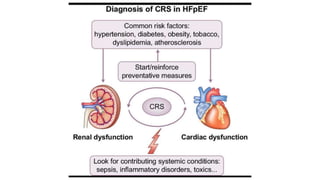
The document discusses the link between heart failure with preserved ejection fraction (HFpEF) and chronic kidney disease (CKD), emphasizing the interdependence of heart and kidney functions, termed nephrocardiology. It highlights the complexities in diagnosis, treatment paradigms, and the pathophysiological interactions between the two organs, including different types of cardiorenal syndrome. Recent advancements in diagnostic algorithms and the potential role of SGLT2 inhibitors in treatment are also explored.






































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













