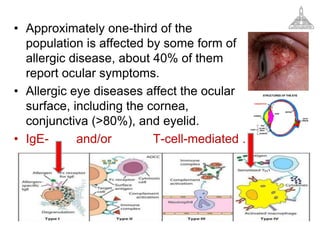
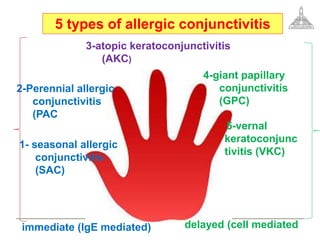
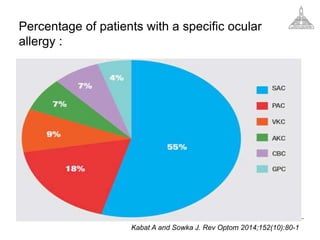
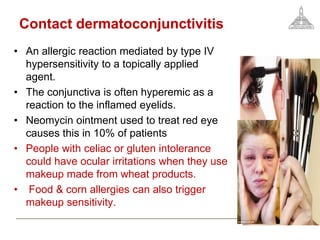
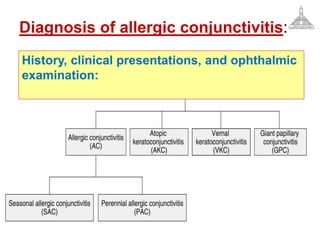
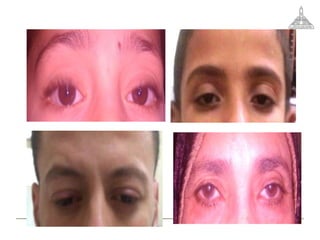


- Ocular allergy affects approximately one-third of the population and manifests as forms including seasonal allergic conjunctivitis, perennial allergic conjunctivitis, vernal keratoconjunctivitis, atopic keratoconjunctivitis, giant papillary conjunctivitis and contact dermatoconjunctivitis. - These forms are mediated by type I and type IV hypersensitivity reactions and have symptoms of itching, redness, burning and watery discharge. - Treatment involves identifying allergens, avoiding triggers, using antihistamines, mast cell stabilizers, NSAIDs and corticosteroids, with immunotherapy and anti-IgE therapy for more severe cases























































































