

![• References
1. Metsala J, Lundqvist A, Virta LJ, et al. The association between asthma and type 1 diabetes: a
paediatric case-cohort study in Finland, years 1981-2009 [published online December 2,
2017]. Int J Epidemiol.
2. Cardwell CR, Shields MD, Carson DJ, et al. A meta-analysis of the association between
childhood type 1 diabetes and atopic disease. Diabetes Care 2003; 26:2568–2574.
3. Cakir M, Akcay S, Karakas T, et al. Prevalence of atopy in children with type 1 diabetes mellitus,
hepatitis B virus carriers, and healthy children: role of T helper 1 (Th1)-type immune
response. Allergy Asthma Proc 2008; 29:166–170. 7.
4. Tzeng ST, Hsu SG, Fu LS, et al. Prevalence of atopy in children with type 1 diabetes mellitus in
central Taiwan. J Microbiol Immunol Infect 2007; 40:74–78.
5. Stene LC, Nafstad P. Relation between occurrence of type I diabetes and asthma. Lancet 2001;
357:607–608.
6. Alves C, Diniz AB, Souza MB, et al. Controversies in the association between type 1 diabetes
and asthma. Arq Bras Endocrinol Metabol 2007; 51:930–937.
7. Tedeschi A, Airaghi L. Common risk factors in type 1 diabetes and asthma. Lancet 2001;
357:1622.
8. Marianna R, Olga B, Tzvi B, et al. TH1/TH2 cytokine balance in patient with both type 1 diabetes
mellitus and asthma. Cytokine 2006; 34:170–176.
9. Stanescu DE, Lord K, Lipman TH. The epidemiology of type 1 diabetes in children. Endocrinol
Metab Clin North Am 2012; 41:679–694.
10. Maahs DM, West NA, Lawrence JM, et al. Epidemiology of type 1 diabetes. Endocrinol Metab
Clin North Am 2010; 39:481–497
11. Black MH, Anderson A, Bell RA, et al. Prevalence of asthma and its association with glycemic
control among youth with diabetes. Pediatrics 2011; 128:e839–e847.
12. Walter RE, Beiser A, Givelber RJ, et al. Association between glycemic state and lung function:
the Framingham Heart Study. Am J Respir Crit Care Med 2003; 167:911–916.](https://image.slidesharecdn.com/asthmaanddiabetesfinal-190212055346/85/Asthma-and-diabetes-21-320.jpg)


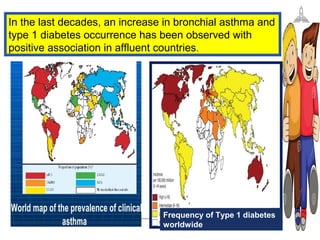
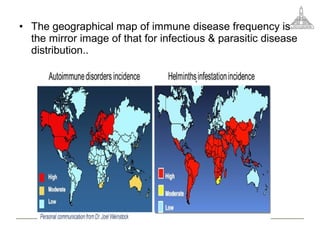
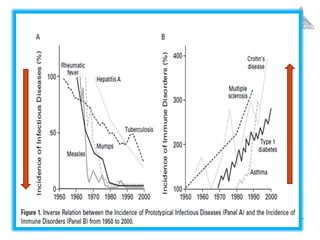
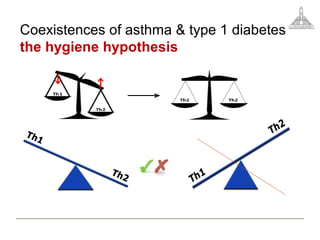
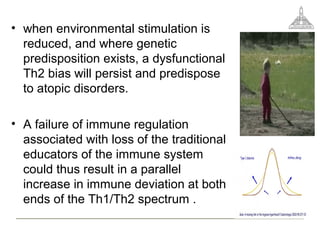
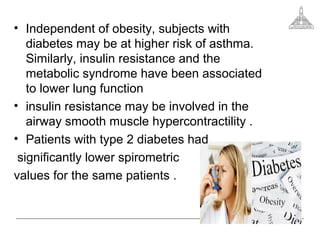
This document discusses the relationship between asthma and diabetes. It notes that both are immune-mediated chronic inflammatory diseases believed to be divergent due to opposing Th1 and Th2 responses. However, altered environmental factors are associated with a growing prevalence of both diseases occurring together. The loss of traditional immune regulators is thought to disrupt the Th1/Th2 paradigm, increasing risk of both allergy and autoimmunity. Immune deficiencies are a major cause of the co-occurrence of asthma and autoimmune diseases like type 1 diabetes. The document also examines links between type 2 diabetes and asthma, as well as interactions between drugs used to treat the conditions.

















![Obesity and diabetes [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/obesityanddiabetesautosaved-151216122724-thumbnail.jpg?width=640&height=640&fit=bounds)























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



