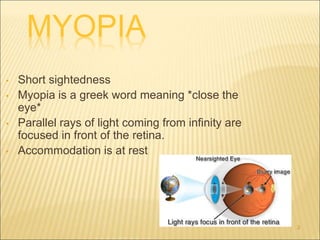
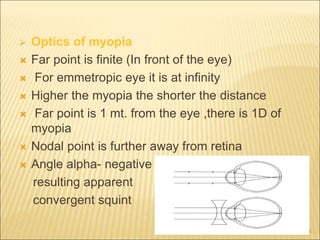
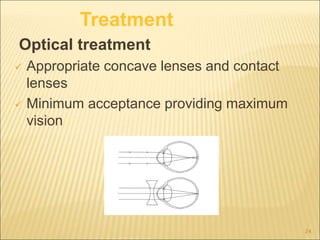
This document discusses myopia (nearsightedness) and its various classifications and treatments. It defines myopia as a condition where parallel rays of light focus in front of the retina. There are several types of myopia classified by factors like age of onset, degree of nearsightedness, and presence of degenerative changes. Treatments include optical correction with glasses or contacts, pharmaceutical agents like atropine to slow progression, and surgical options like LASIK, PRK, and phakic IOL implantation. The goal is to fully correct low to moderate myopia while considering risks of overcorrection for higher degrees of myopia.
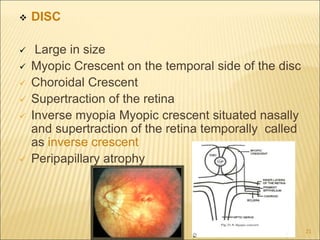

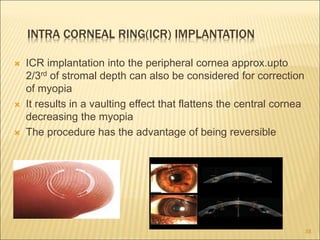
![PHOTOREFRACTIVE KERATECTOMY (PRK)
Involves direct laser ablation of corneal stroma after
removal of corneal epithelium mechanically or
using a laser beam.
Done using Excimer laser
MUNNERLYN EQN: depth of ablation
(micrometer)=[diameter of optical zone(mm)]² ×
1/3power(Diopter)
For myopic a large amount of ablation is done in
central cornea than in the periphery.
Give good results for -2D to -6D of myopia
30](https://image.slidesharecdn.com/myopia-221121163707-23a98b37/85/myopia-ppt-30-320.jpg)
























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






