


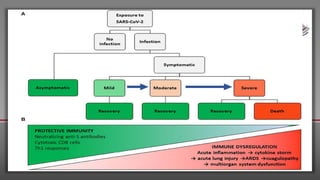





This document discusses COVID-19 in immunocompromised patients. It notes that while immunocompromised patients are at higher risk of severe COVID-19 due to an impaired immune response, the suppression of inflammation may also be protective. The effects of various immunocompromising conditions like HIV, cancer, transplant recipients, and primary immunodeficiencies on COVID-19 outcomes are reviewed. Management strategies like antiviral therapy and immunoglobulin replacement are also discussed. More research is still needed to understand how immunocompromise impacts COVID-19 severity.




















![Novel Corona virus [COVID-19]](https://cdn.slidesharecdn.com/ss_thumbnails/novelcoronaviruscovid-19-200329151226-thumbnail.jpg?width=640&height=640&fit=bounds)
















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






