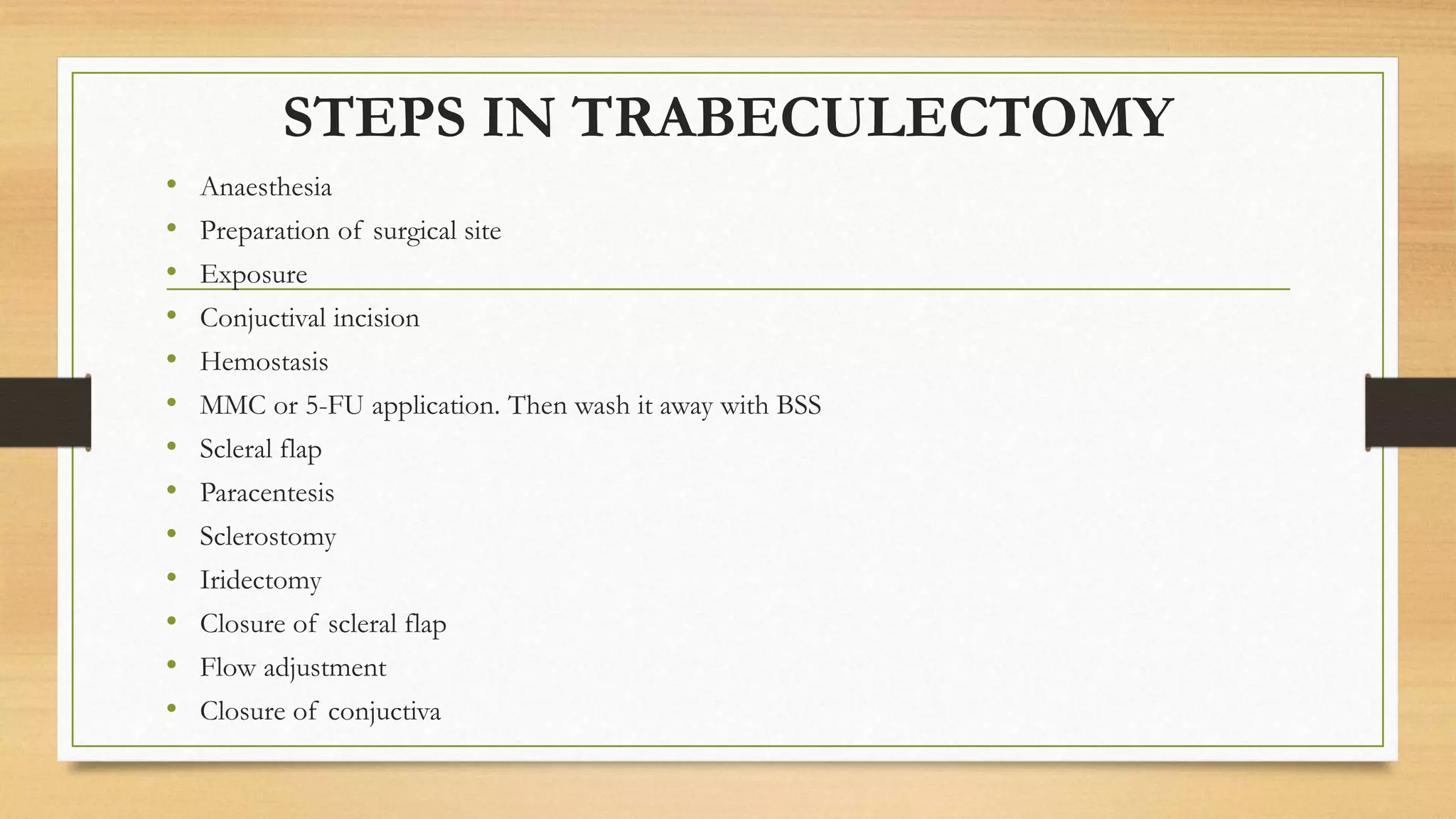
1) Trabeculectomy is a glaucoma surgery that creates an opening in the eye to drain fluid from the anterior chamber and reduce intraocular pressure.
2) It involves making a partial thickness scleral flap, removing a block of tissue underneath, and suturing the flap loosely to allow fluid drainage.
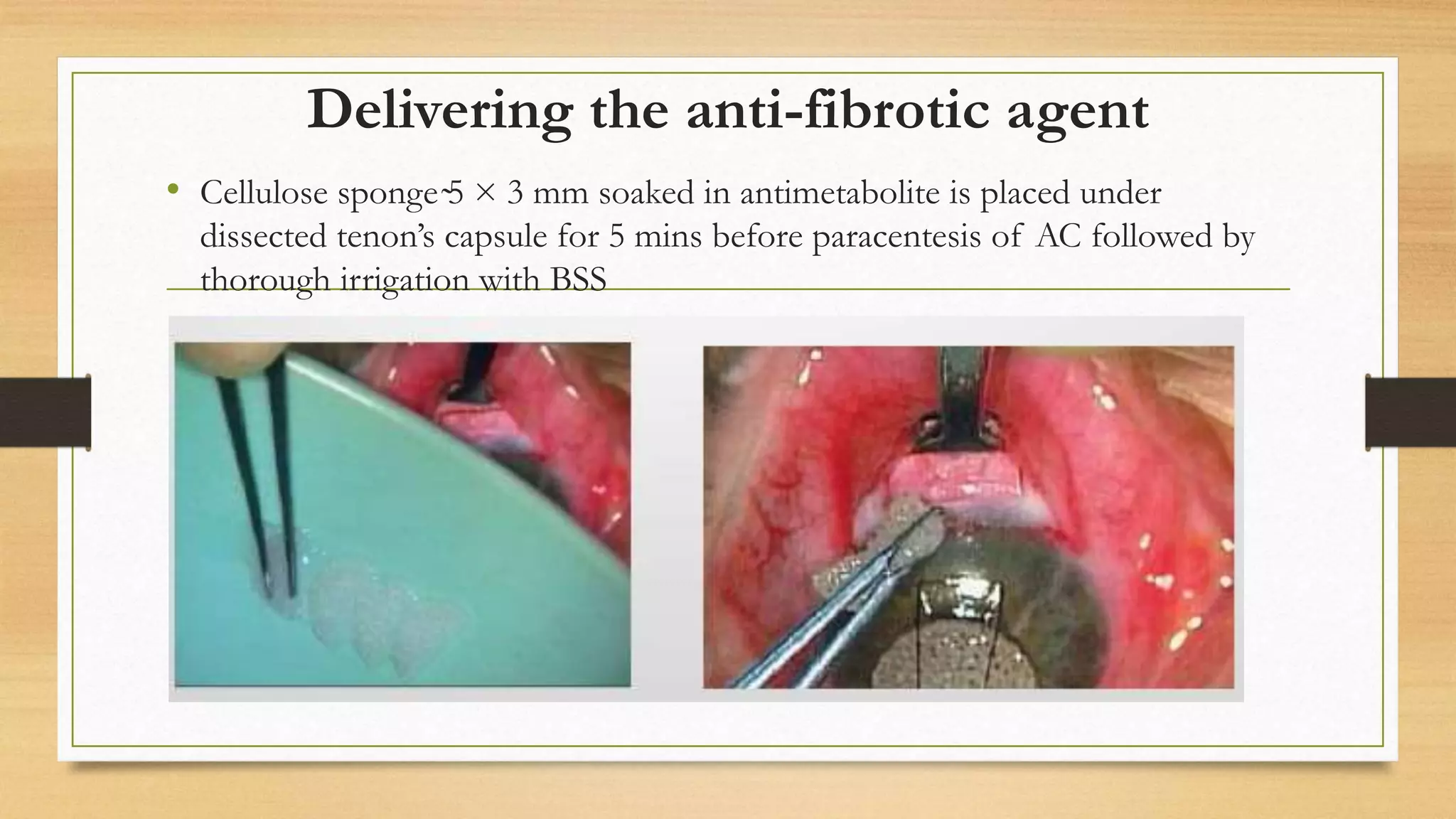
3) Antifibrotic agents like mitomycin C or 5-fluorouracil are often applied to reduce scarring and improve surgical success rates.