Download as PDF, PPTX











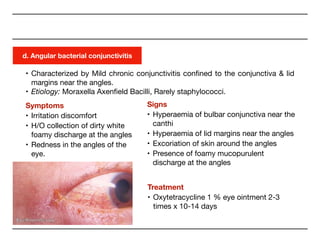



























The document covers conjunctivitis, an inflammation of the conjunctiva categorized into viral, bacterial, and allergic types. It details symptoms, predisposing factors, and treatment approaches for various forms of conjunctivitis. It emphasizes the importance of hygiene in prevention and describes treatment options including antibiotics and topical therapies.