
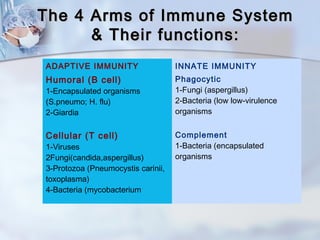
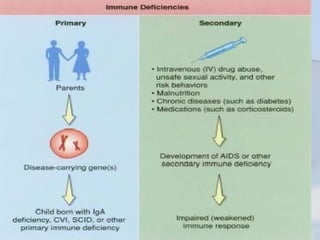
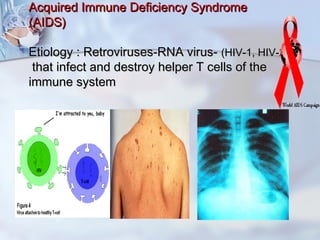
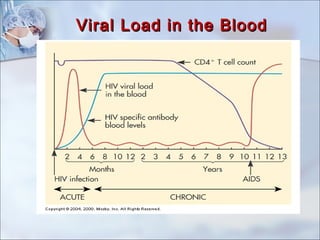
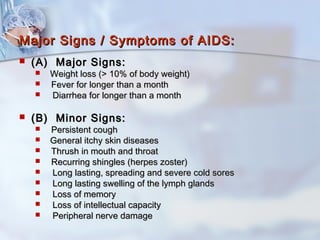
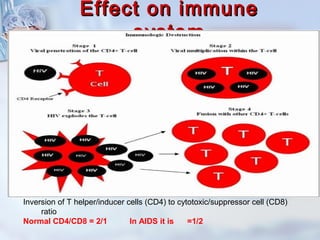
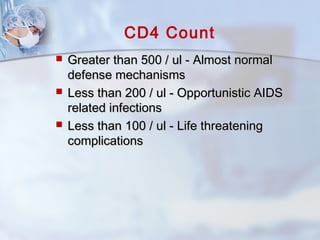
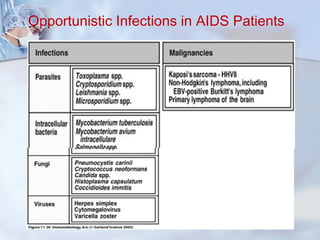
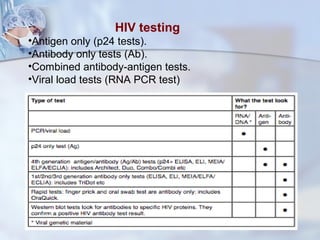



This document discusses acquired immunodeficiency and AIDS. It describes the four arms of the immune system, including innate and adaptive immunity. It defines immunodeficiency as a state where the immune system is compromised or absent, increasing risk of infection and malignancy. It then discusses several causes of secondary immunodeficiency, including AIDS, cancer/chemotherapy, diabetes, transplant immunosuppression, autoimmune diseases, steroid use, asplenia, and aging. For AIDS specifically, it covers the HIV virus, transmission, testing, stages of infection, effects on CD4 counts and the immune system, opportunistic infections, and prevention methods.






















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
