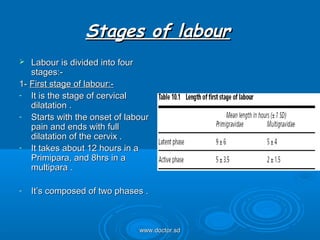
Normal labour involves a series of events that expel the fetus from the uterus through the vagina. It is considered normal when it is spontaneous, occurs at term with a single fetus in vertex presentation, has no undue prolongation, and no maternal or fetal complications. Labour is divided into stages - the first stage involves cervical dilation until full dilation, the second stage is expulsion of the fetus, and the third stage involves delivery of the placenta. Uterine contractions and retraction are the primary forces that cause cervical dilation and expulsion of the fetus, while voluntary abdominal muscle contractions aid in the second stage.