The document discusses normal menstruation, including:
1) Menstruation is the shedding of the endometrium due to declining estrogen and progesterone levels caused by the regression of the corpus luteum.
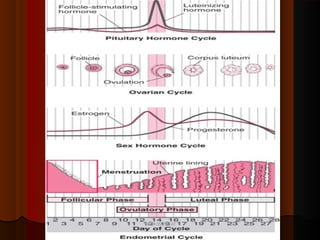
2) The hypothalamic-pituitary-ovarian axis regulates the menstrual cycle through hormones like GnRH, FSH, LH, estrogen and progesterone.
3) A normal menstrual cycle is 28 days, with bleeding typically lasting 3-7 days.