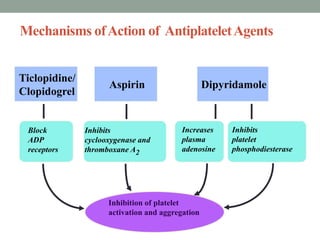
1. Platelets play an important role in both normal hemostasis and pathological thromboses like myocardial infarction and stroke. Antiplatelet drugs are commonly used to prevent strokes.
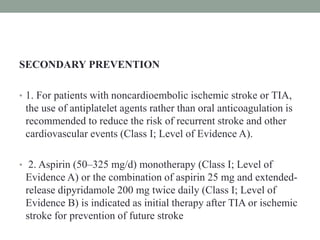
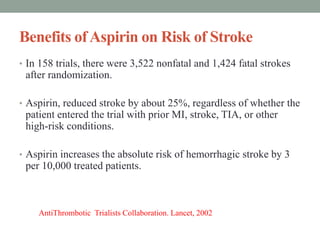
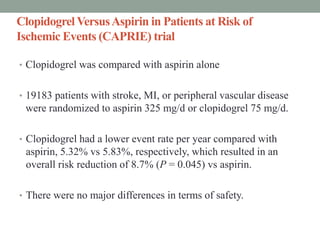
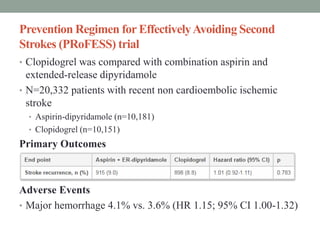
2. Aspirin is recommended for both primary and secondary stroke prevention. Clopidogrel and dipyridamole are also options for secondary prevention. Combination aspirin/dipyridamole may be better than aspirin alone.
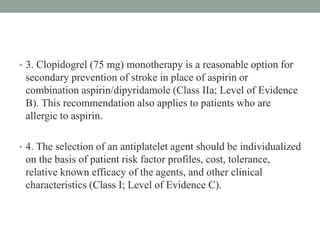
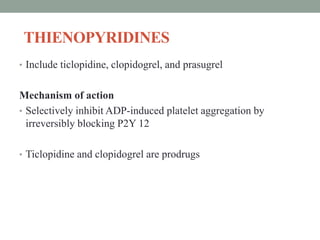
3. Newer antiplatelets like ticagrelor inhibit the P2Y12 receptor more effectively than clopidogrel, but trials found no clear benefit over aspirin for acute stroke. Combining aspirin and clopidogrel long-term increases bleeding risk without

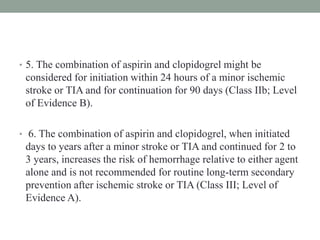
![• In the CSPS ( Cilostazol stroke prevention study) trial of over
1000 patients from Japan, cilostazol (100 mg twice daily)
compared with placebo significantly reduced the risk of stroke
(relative risk reduction 42 percent, 95% CI 9.2-62.5 percent).
• In the CASISP (Cilostazol vs Aspirin for Secondary Ischemic
Stroke Prevention) trial from China of 720 patients with recent
ischemic stroke, the composite endpoint (any stroke, ischemic
or hemorrhagic) at 12 to 18 months of follow-up was lower in
the cilostazol group compared with the aspirin group (3.3 versus
5.6 percent, hazard ratio [HR] 0.62, 95% CI 0.30-1.26) but this
result was not statistically significant](https://image.slidesharecdn.com/neweranti-plateletinstroke-160808113551/85/Newer-anti-platelet-in-stroke-53-320.jpg)







![Management of acute ischemic stroke including tia [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/managementofacuteischemicstrokeincludingtiaautosaved-180808183403-thumbnail.jpg?width=640&height=640&fit=bounds)







![Mechanical thrombectomy in acute stroke [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mechanicalthrombectomyinacutestrokeautosaved-230102142009-fe15766f-thumbnail.jpg?width=640&height=640&fit=bounds)

























































![DUAL AND TRIPLE ANTITHROMBOTIC THERAPY FOR SECONDARY STROKE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dualandtripleantithrombotictherapyforsecondarystrokeautosaved-230904113552-c3502b37-thumbnail.jpg?width=640&height=640&fit=bounds)

































