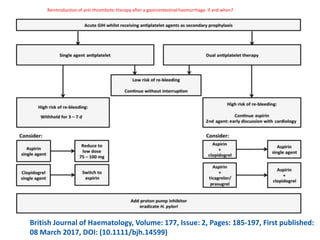
- Aspirin is recommended within 24-48 hours for acute ischemic stroke (AIS) and after 24 hours if IV thrombolysis is administered.
- For minor strokes, dual antiplatelet therapy with aspirin and clopidogrel for 21 days begun within 24 hours is recommended, followed by clopidogrel alone for 90 days.
- The efficacy of IV antiplatelet drugs like tirofiban and eptifibatide for AIS is not well established and requires further research.














































![PHARMACOTHERAPY POINTERS FOR ISCHEMIC STROKE [MALAYSIAN CPGs].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/pharmacotherapypointersforischemicstrokemalaysiancpgs-230519035129-300dc0e5-thumbnail.jpg?width=640&height=640&fit=bounds)

![DUAL AND TRIPLE ANTITHROMBOTIC THERAPY FOR SECONDARY STROKE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dualandtripleantithrombotictherapyforsecondarystrokeautosaved-230904113552-c3502b37-thumbnail.jpg?width=640&height=640&fit=bounds)






































