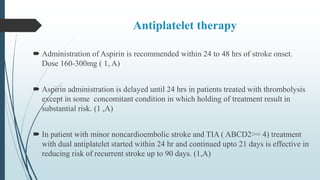
1. Regional stroke centers should be established to provide thrombolysis and transport to endovascular treatment centers. Every hospital should have a stroke team and protocols for emergency evaluation.
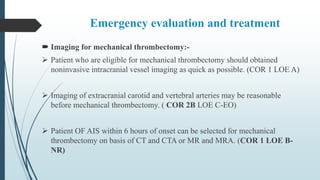
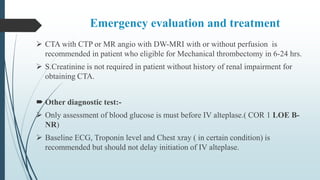
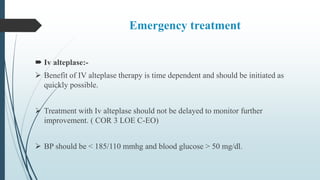
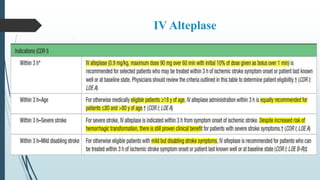
2. Patients should receive IV alteplase as quickly as possible if eligible. Mechanical thrombectomy is recommended for large vessel occlusions within 6-24 hours of onset depending on criteria.
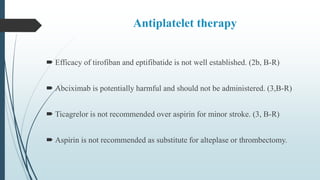
3. In-hospital prevention includes antiplatelet therapy, vascular imaging, and lipid management with statins to reduce cardiovascular risk.









![Management of acute ischemic stroke including tia [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/managementofacuteischemicstrokeincludingtiaautosaved-180808183403-thumbnail.jpg?width=640&height=640&fit=bounds)













































![DUAL AND TRIPLE ANTITHROMBOTIC THERAPY FOR SECONDARY STROKE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dualandtripleantithrombotictherapyforsecondarystrokeautosaved-230904113552-c3502b37-thumbnail.jpg?width=640&height=640&fit=bounds)

































