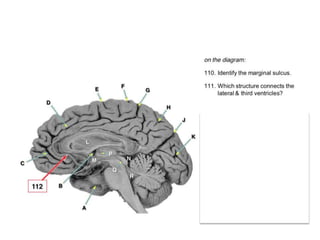
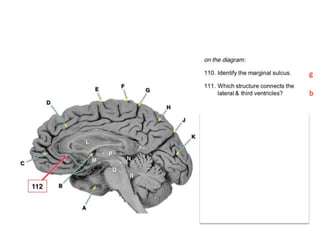
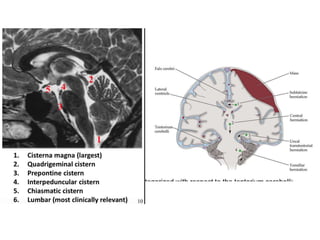
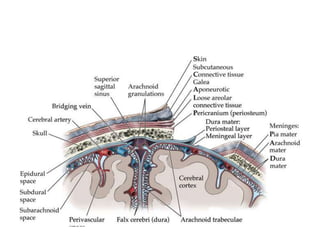
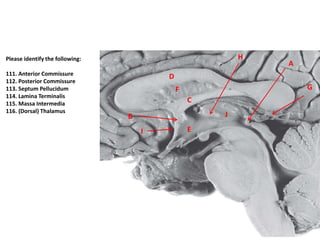
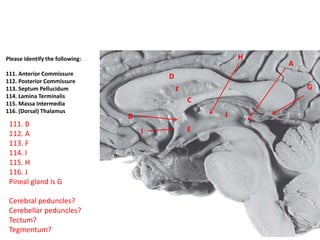
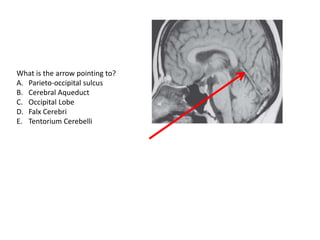
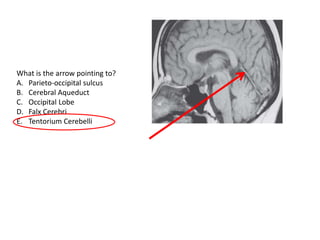
The document discusses various topics related to neuroscience and the brain. It includes questions about different types of brain imaging techniques, CNS structures and their locations, brain development, and cell types in the brain. It also covers topics like functional MRI, spinal anesthesia, brain injuries, and the differences between the central and peripheral nervous system responses to injury.














































![0001 Neurophysiology 0001[Recovered].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/01neurophysiology0001recovered-250210163121-35929a9a-thumbnail.jpg?width=640&height=640&fit=bounds)































