This document provides an overview of cranial computed tomography (CT) for medical undergraduates, detailing its principles, mechanism, advantages over MRI, and various clinical applications including head trauma, cerebrovascular accidents, and CNS infections. Key concepts such as the Hounsfield unit, different window levels for brain imaging, and anatomical structures visible in CT scans are discussed. It emphasizes the critical role of CT in emergency medicine, particularly for assessing neurological conditions.
![Extradural hemorrhage
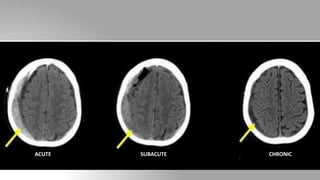
• Location: Between the inner surface of skull and outer layer of dura
(periosteum)
• As a result, EDHs are usually limited in their extent by the cranial
sutures [unlike SDH, which are not limited by sutures]
• Features in CT: Biconvex in shape, hyperdense, sharply demarcated
• Features of mass effect (i.e. midline shift and uncal herniation) may
be present.](https://image.slidesharecdn.com/essentialsofctbrainforundergraduate-220920175038-e86e9a55/85/ESSENTIALS_OF_CT_BRAIN_For_Undergraduate-pptx-18-320.jpg)



















































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)















