Downloaded 113 times






























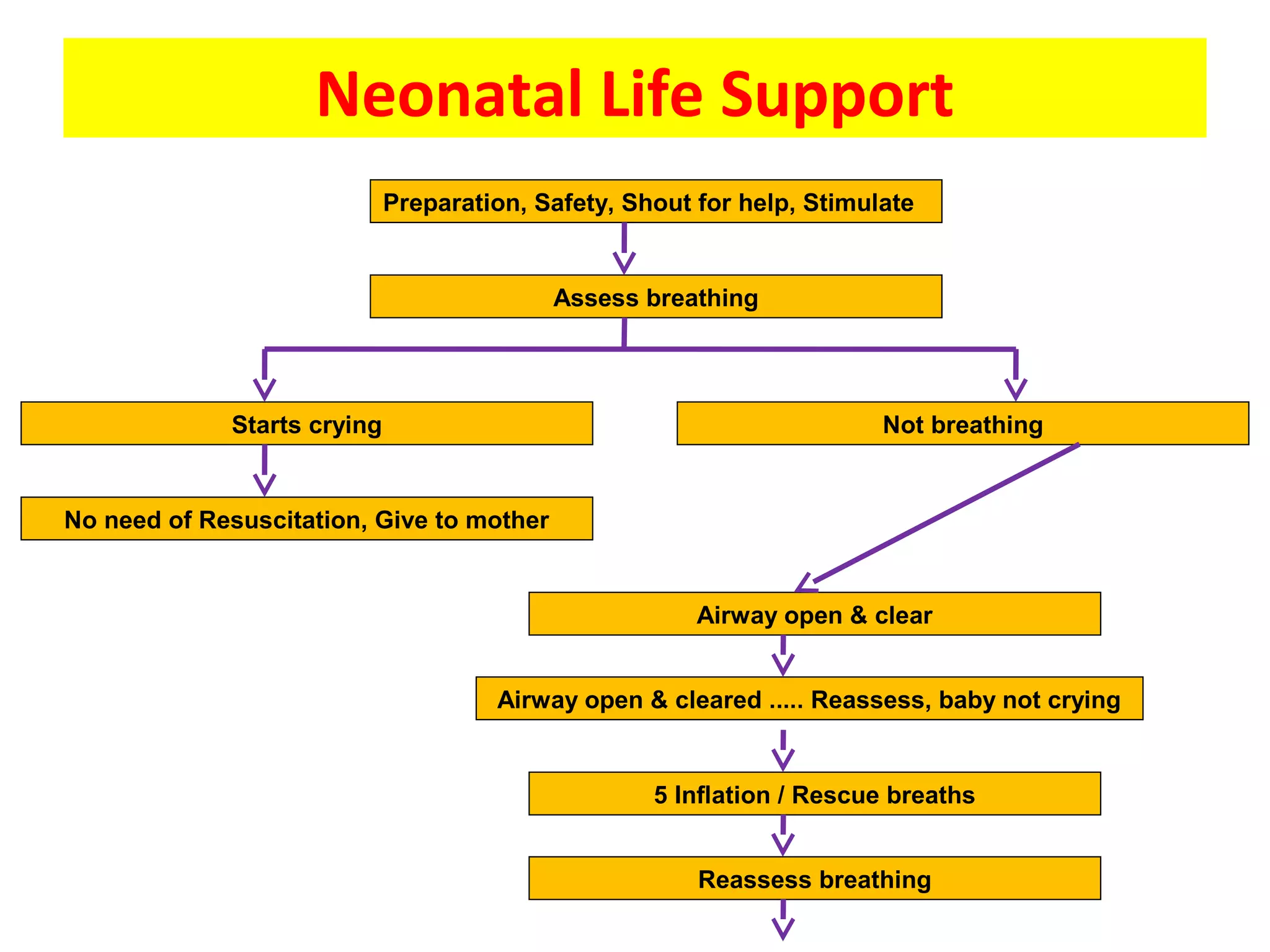

















This document provides guidance on neonatal resuscitation. It states that about 10% of newborns require assistance breathing after delivery, and under 1% require extensive resuscitation. Basic resuscitation involves airway support and breathing/ventilation, while advanced resuscitation adds chest compressions, intubation, cannulation, and drugs. It outlines the steps of neonatal resuscitation including preparation, stimulation, assessing breathing, airway management, ventilation, chest compressions if needed, and post-resuscitation care. Key equipment and medications are also listed.







































































































