Clinical Findings ofAbnormal Transition (Fetal
to neonatal Transition)
• Irregular breathing, absent breathing (apnea), or rapid breathing
(tachypnoea)
• Slow heart rate (bradycardia) or rapid heart rate (tachycardia)
• Decreased muscle tone.
• Pale skin (pallor) or blue skin (cyanosis).
• Low oxygen saturation.
• Low blood pressure.
3.
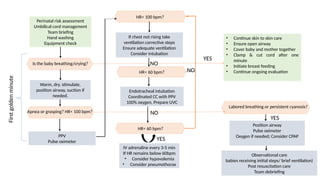
• Continue skinto skin care
• Ensure open airway
• Cover baby and mother together
• Clamp & cut cord after one
minute
• Initiate breast feeding
• Continue ongoing evaluation
PPV
Pulse oximeter
HR< 100 bpm?
If chest not rising take
ventilation corrective steps
Ensure adequate ventilation
Consider intubation
Apnea or grasping? HR< 100 bpm?
Endotracheal intubation
Coordinated CC with PPV
100% oxygen, Prepare UVC
IV adrenaline every 3-5 min
If HR remains below 60bpm
• Consider hypovolemia
• Consider pneumothorax
Perinatal risk assessment
Umbilical cord management
Team briefing
Hand washing
Equipment check
Warm, dry, stimulate,
position airway, suction if
needed.
Is the baby breathing/crying?
Labored breathing or persistent cyanosis?
Position airway
Pulse oximeter
Oxygen if needed; Consider CPAP
Observational care
babies receiving initial steps/ brief ventilation)
Post resuscitation care
Team debriefing
NO
NO
HR< 60 bpm?
HR< 60 bpm?
First
golden
minute
YES
YES
NO
YES
4.
Preparation for Birth
•Any Birth is a potential Birth Emergency.
• According to the 7th
Edition:
1. What is the expected gestational age?
2. Is the amniotic fluid clear?
3. How many Babies?
4. Any Additional risk factors?
5.
• Changes in8th
edition:
1. What is the expected gestational age?
2. Is the amniotic fluid clear?
3. Additional risk factors
4. Umbilical cord management plan.
6.
Antenatal Risk factors
•Gestational age < 37 week or >41
week.
• Maternal hypertension
• Pre eclampsia or eclampsia.
• Multiple gestation.
• Polyhydramnios or
oligohydramnios
• IUGR.
• Significant foetal malformation.
• No antenatal Care
• Foetal hydrops
Intrapartum Risk factors
• Emergency LSCS
• Forceps or Vacuum Assisted
delivery
• Breach or other abnormal
presentation
• Foetal bradycardia(category 2 and
3)
• Intrapartum Bleeding
• Meconium stained liquor
• Placental abruption
• Maternal General anaesthesia or
Mg Therapy
• Shoulder dystocia
7.
• Assess riskfactors.
• Identify team leader.
• Anticipate potential complications and plan a team response.
• Delegate tasks.
• Identify who will document events as they occur.
• Determine what supplies and equipment will be needed.
• Identify how to call for additional help.
Pre-resuscitation Team Briefing
8.
How Many personalin Resuscitation Team
• No risk factor : At least 1 who is trained in NRP, and able to initiate
PPV
• If any Risk factors identified: At least 2 or more who is trained in
NRP, with one person trained in advanced NRP
9.
If the Babyis crying and breathing
• Keep the baby on Mothers abdomen with an intact umbilical cord
• Dry and remove wet cloth
• Skin to skin contact
• Secretions: suction
• Ongoing evaluation
• Initiate breastfeeding.
10.
INITIAL STEPS OFRESUSCITATION
in 7th
edition
If the Baby is not crying or breathing or having gasping respiration at birth,
Initial steps are required
Clamp and Cut the cord and transfer the baby to the radiant warmer
• Warm and maintain normal temperature.
• Position airway.
• Clear secretions if needed.
• Dry and stimulate
11.
• Now in8th
edition
• Dry the baby and remove the wet linen.
• Stimulate the baby by Gently rubbing the back and extremities.
• Position the Head and Neck to open the Airway, may use a
shoulder role to maintain correct position. (Sniffing the
morning air position).
• Clear Secretions from mouth and nose if required. Mouth f/by
nose. 5 cm max for mouth and 2 cm for nose. Apply suction
while withdrawing the tube, Max pressure of 80 to 100 mmHg
12.
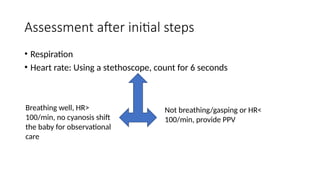
Assessment after initialsteps
• Respiration
• Heart rate: Using a stethoscope, count for 6 seconds
Breathing well, HR>
100/min, no cyanosis shift
the baby for observational
care
Not breathing/gasping or HR<
100/min, provide PPV
13.
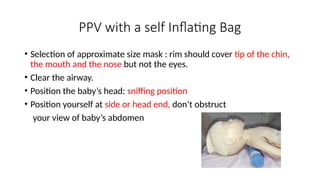
PPV with aself Inflating Bag
• Selection of approximate size mask : rim should cover tip of the chin,
the mouth and the nose but not the eyes.
• Clear the airway.
• Position the baby’s head: sniffing position
• Position yourself at side or head end, don’t obstruct
your view of baby’s abdomen
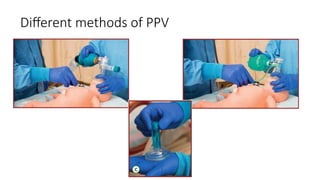
14.
• Mask isheld on face with thumb, index and/or middle finger ; forming the shape
of the letter C, while ring and fifth finger bring the chin forward.
• Gentle downward pressure to form an airtight seal.
15.
• Initiation ofventilation: squeeze the bag to produce a gentle chest
rise.
• First few breaths require higher pressures and longer inflation times.
• Rate 40 to 60/min, Try saying Breathe… two…. Three…
• Room air for babies >/= 35 weeks, 21 to 30% for < 35 weeks.
Baby is reassessed after 15 seconds for effective PPV
16.
Effective PPV
• Assessedafter 15 seconds
• Increases HR
• Chest moving with PPV
Ineffective PPV
• Corrective Actions- MR SO P A
• Five rescue breaths with each step to assess chest
movement with PPV
• MR Mask readjustment, Reposition the head and
Neck
• SO Suction the mouth and Nose, Open the mouth
• P Increase the pressure by squeezing the bag
harder. increase in 5-1 O cm H20 increments to
maximum recommended pressure.
• Max 40 cm H20 term
• Max 30 cm H20 preterm
• A Alternate airway like intubation.
• After 30seconds of effective ventilation assess for spontaneous
breathing and Heart rate.
• If the Heart rate > 100/min, continue ventilation till spontaneous
respiration starts; Gradually taper and stop.
• Check for O2 saturation, If saturation below target range, provide free
flow oxygen.
• Laboured Breathing: CPAP, Not used for gasping respiration.
• 60>HR<100/min:
a. If HR is increasing continue ventilation and adjust fio2.
b. If HR not raising check for chest raise
c. Chest not raising, consider intubation.
d. HR<60/min, Check for chest raise, Intubate.
19.
Endotracheal Intubation
• Indicationfor endotracheal Intubation.
i. HR<100, and not increasing despite providing PPV.
ii. Requirement of Surfactant administration and suspicion of Diaphragmatic
hernia.
iii. Prolonged PPV
iv. Recommended before started CC.
• Size of ET: Weight Gestational Age ET No
Below 1 kg <28 weeks 2.5
1 to 2 kg 28 to 32 weeks 3
> 2kg >34 weeks 3.5
20.
• In the7th
edition
• An electronic cardiac
monitor is the preferred
method for assessing heart
rate during cardiac
compressions.
• In the 8th
edition
• When an alternative airway
becomes necessary, a cardiac
monitor is recommended for
the most accurate assessment
of the baby’s heart rate.
21.
Chest Compressions andmedications.
• Chest compressions are indicated if HR<60/min despite 30 seconds of
effective ventilation.
• Technique:
1. Head End.
2. Apply pressure on lower third of the sternum, below imaginary line connecting baby’s
nipple.
3. Encircle the baby’s chest within your hand, and support back with your fingers
4. Thumbs on centre of sternum
5. Depth: at least 1/3rd
of anteroposterior diameter.
6. Rate: 90/min.
7. Compression ventilation ratio of 3:1.
• Re evaluate after 60 seconds.
22.
• CARDIO forreassessment:
1. C - chest moving with PPV.
2. A – airway secured by ET
3. R – Rate of CC to ventilation
4. D – correct Depth of compression.
5. IO – inspired oxygen concentration is 100%.
• HR>60/min, stop chest compressions and continue ventilation at a
rate of 40 to 60 breaths/min, FiO2 titrated ac/to target Spo2
• Reassessed after every 30 seconds
23.
Medications
• Medications Required:
1.Adrenaline
2. Volume expander.
• Indications: HR < 60/min even after at least 30 seconds of effective ventilation
f/by 60 seconds of coordinated compressions ventilations with 100% oxygen.
• Routes of administration:
1. Intravenous 0.2ml/kg of body weight of 1:10000 solution (Range 0.1-0.3ml/kg)
2. Intraosseous same as intravenous
3. Endotracheal 1 ml/kg of body weight of 1:10000 (range 0.5ml – 1 ml/kg) f/by
several positive pressure breaths.
• Followed by saline.
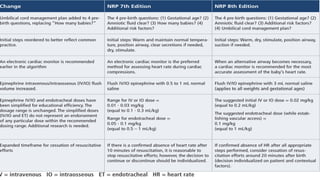
24.
In 7th
edition
• Rangefor IV or IO dose = 0.01 -
0.03 mg/kg (equal to 0.1 - 0.3
mL/kg)
• Flush IV/IO epinephrine with 0.5
to 1 mL normal saline.
• Range for endotracheal dose =
0.05 - 0.1 mg/kg (equal to 0.5 – 1
mL/kg)
In 8th
edition
• The suggested initial IV or IO
dose = 0.02 mg/kg (equal to 0.2
mL/kg).
• Rapid administration f/by 3 ml of
saline( applies to all weights).
• The endotracheal dose (while
establishing vascular access) =
0.1 mg/kg (equal to 1 mL/kg)
25.
• After Adrenalinecontinue ventilation and coordinated chest
compressions, reassess after 60 seconds.
• Repeat adrenaline after 3 to 5 minutes.
• If the HR persistently remains <60 consider hypovolemic shock or
Tension pneumothorax.
26.
VOLUME EXPANDERS
• Indications:
1.Baby not responding to steps of resuscitation.
2. Signs of shock or
3. History of blood loss.
• Volume expanders used are:
1. Normal saline.
2. PRBC non cross matched type O rh negative blood.
• 10ml/kg to be given over 5 to 10 minutes, Repeated once for non
responders.
27.
Changes regarding whento stop:
7th
edition
• confirmed absence of heart rate
after 10 minutes of
resuscitation.
• Decision is individualized.
In 8th
edition
• consider cessation of
resuscitation efforts around 20
minutes after birth.
• decision individualized on
patient and contextual factors
28.
WHEN TO STOP
•When the HR is absent after 20 minutes despite performing all
resuscitation steps.
• Post Resuscitation care: Close monitoring and frequent assessment of
1. Respiratory effort.
2. Oxygenation.
3. Blood glucose
4. Electrolytes
5. Urine output
6. Neurological status and
7. Temperature monitoring.