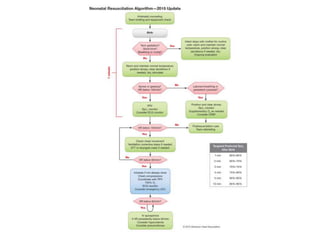
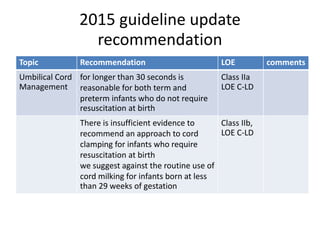
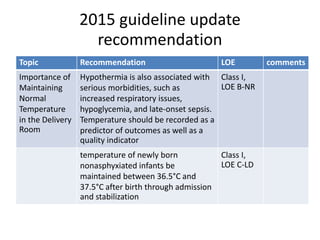
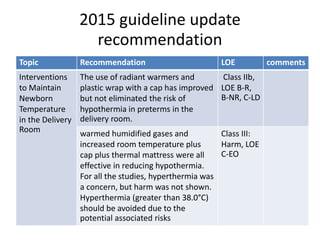
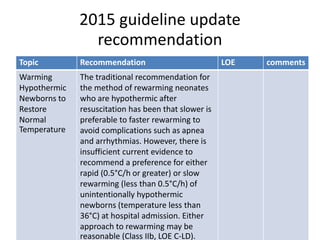
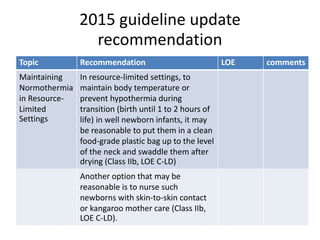
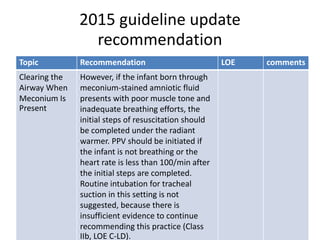
This document provides recommendations from the 2015 Neonatal Resuscitation Guidelines on various topics relating to neonatal resuscitation. It discusses recommendations regarding umbilical cord management, maintaining normal temperature, warming hypothermic newborns, administration of oxygen, positive pressure ventilation, and other aspects of resuscitation. The recommendations are based on levels of evidence and aim to optimize resuscitation practices for improved newborn outcomes.