Download to read offline
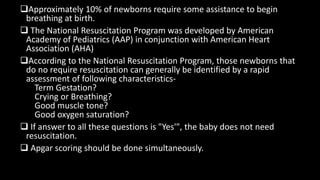
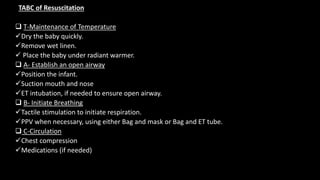


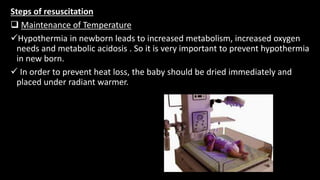
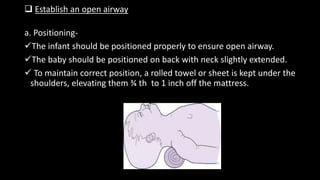

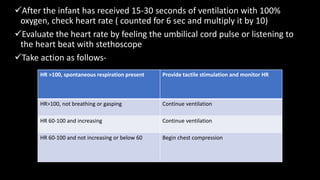
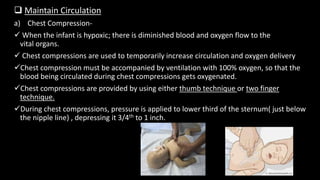
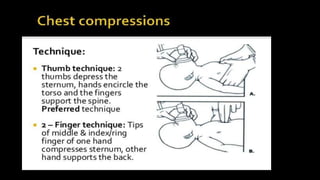
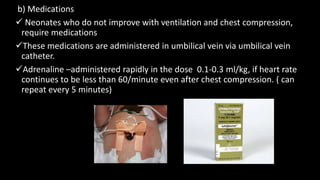
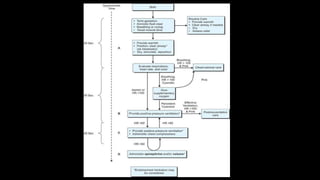

The document discusses neonatal resuscitation guidelines from the American Academy of Pediatrics. It outlines the assessment of newborns to determine if resuscitation is needed, including checking gestation, crying, muscle tone, oxygen saturation and Apgar score. The steps of resuscitation include maintaining temperature, establishing an open airway through positioning and suctioning, initiating breathing through tactile stimulation or positive pressure ventilation, and maintaining circulation through chest compressions and potentially medications if the heart rate does not improve. Equipment, medications and proper techniques are described for each step of resuscitation.



































































